Electronic ISSN 2287-0237
Thoracic Outlet Syndrome (TOS) is not a common disease in Asian populations. The patients normally present with symptoms from external compression of subclavian artery, subclavian vein, and brachial plexus, which might mimic other more common conditions. Compression could be from conditions such as trauma to the first rib, anatomical pathology, repetitive injury from activity causing scar formation and compression of those structures. The correct diagnosis requires additional tests such as magnetic resonance image (MRI), electromyography (EMG), and/or Computed Tomography (CT) angiogram. The mainstay of treatment is a procedure called first rib resection, which can be performed via many approaches such as anterior approach1, supraclavicular2, transaxillary approach2-3, thoracoscopic approach.4-5 Anterior and supraclavicular approach provides excellent exposure around first rib area but has cosmetic concerns. Transaxillary approach also provides good surgical exposure but can be technically challenging in obese patients. Thoracoscopic approach is the least invasive but has poor exposure above rib and scalene muscle. This case is a non-athletic young female without any history of trauma or such repetitive activity involving the interscalene area. She developed TOS symptom after underwent transaxillary breast implantation. First rib resection via transaxillary approach was performed to alleviate the patient symptoms.
A 30-year-old Asian female, slender build, with a history of deep invasive endometriosis and bilateral breast implantation 2 years ago via axillary incision, presented with numbness, tingling and weakness of right hand for 2 months. She complained of the inability to put on make-up properly as an initial symptom. She was evaluated by an orthopedist who attempted to perform steroid injection at her wrist without clinical improvement. Upon physical examination, it revealed severe atrophy of right thenar and hypothenar muscle as well as weakness of intrinsic muscle of hand (Figure 1). It also showed numbness of right hand and distal forearm. Her radial pulse became absent upon neck extension and ipsilateral neck rotation. EMG demonstrated acute denervation and severe motor axonal loss at right C8-T1 innervated muscles with absent right medial antecutanous responses, compatible with right lower trunk brachial plexopathy. MRI in neutral neck position revealed presence of right elongated C7 transverse process with narrowing of inferior portion of scalene triangular space with probable compression of right brachial plexus (Figure 2), therefore, she was diagnosed with combined neurogenic and arterial Thoracic Outlet Syndome (nTOS and aTOS). All findings were discussed with the patient and she elected to proceed with surgical resection of first rib via trans- axillary approach.

Figure 1: Images show severe atrophy of intrinsic muscle of right hand.
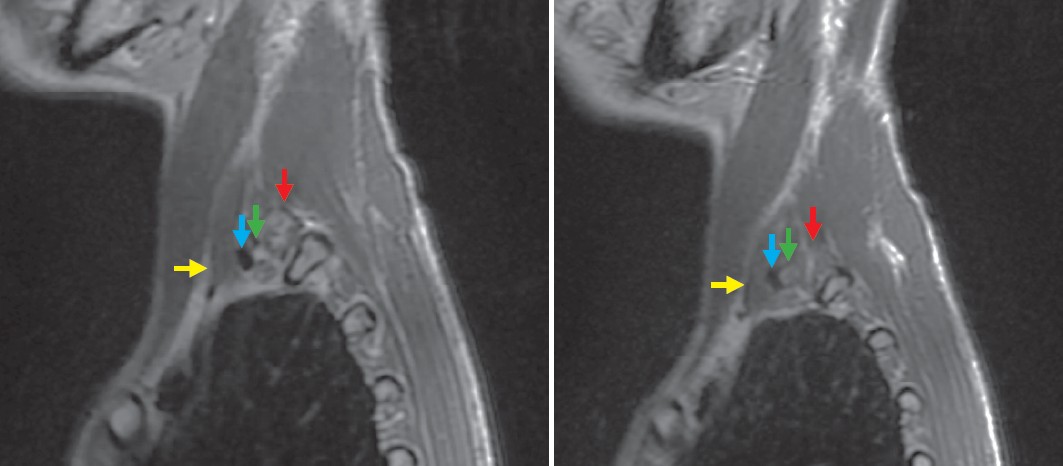
Figure 2: Elongated C7 transverse process compressing right subclavian artery (RSCA) and brachial plexus.
Red arrow = elongated C7 transverse process
Blue arrow = compression of right subclavian artery (RSCA)
Green arrow = brachial plexus
Yellow arrow = anterior scalene muscle
In the operating theater, general anesthesia was performed by single lumen endotracheal tube. The patient was positioned on full left lateral decubitus with abduction of right arm (swimming position) in order to fully expose right axilla. Usual incision is a transverse incision below axillary hairline between pectoralis major and latissimus dorsi, but since the patient already had previous 5 cm semi transverse incision from breast implant at 1.5 cm below of axillary triangle, incision was made over the previous one due to cosmetic concerns. Old, thick scarring was encountered in the surgical area. The dissection was carried over to chest wall with care to not injure the intercostobrachial nerve. Once chest wall was met, subcutaneous and fatty tissue were retracted medially and laterally by Deaver retractor. Fibrous tissue from breast implantation was found around first rib. Periosteum of first rib was then cauterized along its course, Adson periosteal elevator was used to peel it away from bony part superiorly and inferiorly. Doyen rib elevator was then used to encircle the rib anteriorly and posteriorly. Subclavian artery was identified just behind the scalene anterior then it was mobilized away from subclavian
vein anteriorly. During dissection, we preferred not to use cauterization both monopolar and bipolar due to abundant nerve supply in the area. Division and resection of scalene anterior was performed using Metzenbaum after elevation of muscle by right angle followed by scalene medius and subcla- vius in the same fashion (Figure 3). Once scalene muscles were resected, Doyen rib elevator was used to free up to the rib from surrounding tissue. Giertz-Stille rib cutter was used to divide it anteriorly and posteriorly. Remaining rib was removed by Rongeurs anteriorly to cartilaginous part of first rib and pos-teriorly to junction between transverse process and rib (Figure 4). One 16Fr chest drain was placed into pleura, which was removed on postoperative day 1, and patient was discharged home later that day. Upon 1 month and 6-month follow-up, patient reported significant improvement in pain and numbness in previously affected area as well as significant improvement in motor power of the right hand. The patient also reported no paresthesia along medial surface of right arm. Adson test was negative. Chest x-ray showed total absent of right first rib without elevation of right hemidiaphragm (Figure 5)
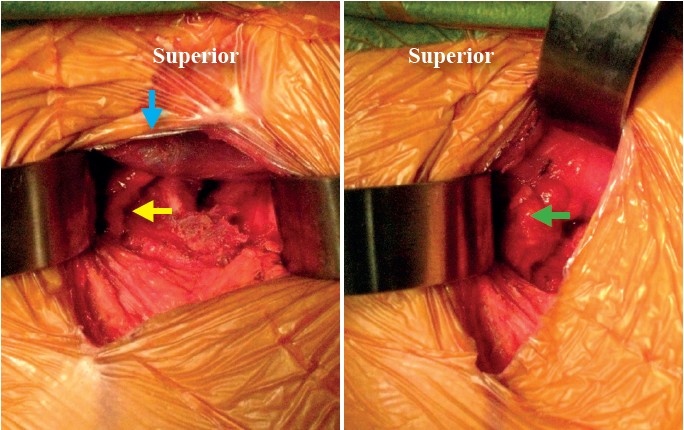
Figure 3: Blue arrow = right subclavian vein (RSCV)
Yellow arrow = right subclavian artery (RSCA)
Green arrow = brachial plexus after retraction of RSCV and RSCA

Figure 4: Resected first rib.
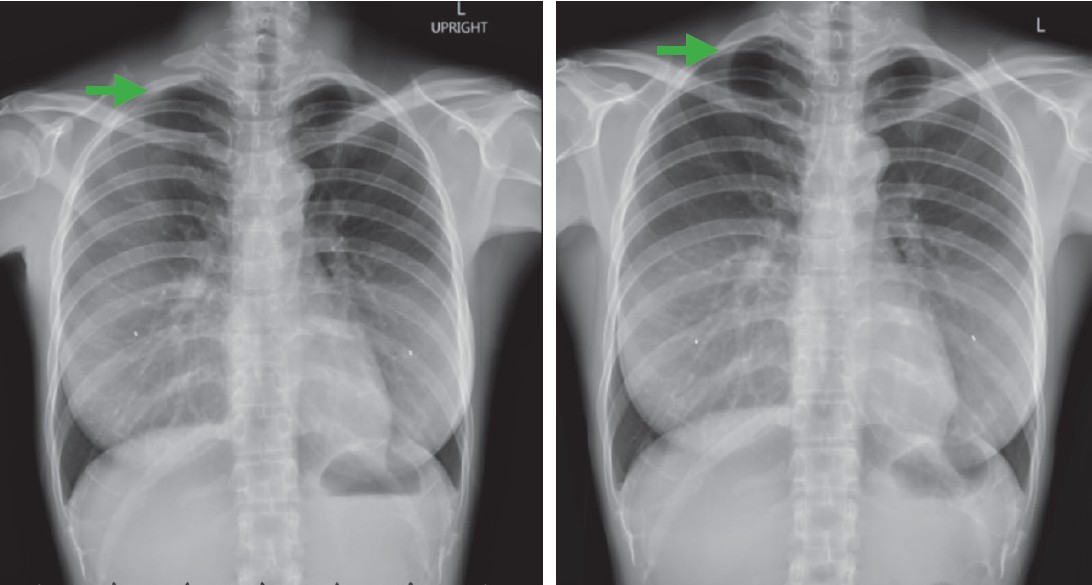
Figure 5: Postoperative chest x-ray (right) shows absence of right first rib.
Combined neurogenic TOS (nTOS) and arterial TOS (aTOS) is a rare condition6 accounting for less than 2% of all TOS, which normally represent pathology in the interscalene triangle from cervical rib or elongated transverse process. Pathophysiology of TOS normally involves repetitive injury around first rib resulting in tightening or scar formation around the first rib, however, surgery around axillary area can also produce scar formation and aggravated symptoms in patients with mild anatomical pathology.
This patient was initially diagnosed with carpal tunnel syndrome without any improvement of steroid injection at median nerve. EMG and MRI played an important role for the diagnosis.7 One must be careful with clinical diagnosis especially with vascular involvement. In aTOS, some cases may present with poststenotic dilatation or aneurysmal change.8 However, it did not present in this case.
Supraclavicular approach was initially described with good outcome but there were concerns of cosmetic and neuropathy from supraclavicular nerve. Urschel described transaxillary approach9,10 as his preferred method for total removal of first rib and all the compression in thoracic outlet area with comparable outcomes in upper and lower brachial plexopathy. We employed this technique on the patient to ensure complete removal of the scar around axillary area. In general, dissection down to first rib in a slender patient is straightforward; however, this patient had previous surgery causing scarring in axillary area, therefore a meticulous technique needed to be performed to ensure safety of vital structures. Raakhi7 reported a case of a ruptured breast implant, then causing bilateral axillary lymphadenopathy which eventually developed into bilateral TOS11, however, lymphadenopathy was not found in this case. Once first rib was resected, dissec- tion was similar to Urschel technique. We were able to achieve the goal of complete removal of first rib as shown in Figure 5. The six-month follow up showed much improvement in muscle power and muscle mass of intrinsic muscle of hand.
The transaxillary approach for first rib resection is a safe and feasible procedure in the case of combined nTOS and aTOS syndrome even in patients who have had previous surgery around axillary region, for instance, breast implantation surgery.









