Electronic ISSN 2287-0237
Carotid artery disease (CAD) is caused by an accu- mulation of cholesterol plaque or atherosclerosis resulting in the thickening of the arterial wall at the intima media layer. Atherosclerotic plaques lead to a reduction in the size of arterial diameters and ultimately stenosis. Large plagues can potentially disrupt arterial blood flow and eventually reduce blood supply to the cerebral hemispheres.1 Carotid plaque is established as an important risk factor for cerebrovascular disease or stroke.2
A systemic review and meta-analysis from 40 studies conducted in subjects worldwide from 1966-2007 revealed that moderate stenosis and more (≥ 50%) were associated with gender and age. In subjects aged less than 70 years old, the prevalence of stenosis was 4.8% in men and 12.5% in women. In subjects aged 70 years and older, the prevalence was 2.2% and 6.9% in men and women respectively.3
In Thailand, a study of extracranial internal carotid artery (ICA) and intracranial artery stenosis in asymptomatic subjects aged 45 years and older revealed that the prevalence of moderate stenosis of the ICA was 1.5% and intracranial artery stenosis was 5%. In people of 60 years and older, HT and ischemic heart disease were associated with plague formation of the extracranial ICA.4
The US Preventive Service Task Force has addressed important risk factors for CAD including aging, male gender, HT, smoking, hyperlipidemia and heart disease. These established risk factors are also related to cardio- vascular disease risk.5 In addition, a study showed that Thai elders with ischemic stroke were 4 times more likely to have moderate to severe carotid arterial stenosis.6 Moreover, people who had 60-99% ICA stenosis would have a likelihood of suffering large artery disease stroke, lacunar or cardioembolic stroke at a rate of 9.9%, 6% and 2.1%, respectively during 5 years.7
The intimal media thickness (IMT) can be used as a predictor for vascular disease. The carotid IMT has been linked to HT and stroke.8 A study of cervical carotid IMT in 5,855 elderly patients, without a history of cardiovascular disease, revealed that for each 0.2mm of common carotid artery (CCA) IMT thickening the risk of ischemic stroke and myocardial infarction increased by 1.27 times and for each 0.55mm of ICA thickening the risk increased by 1.3 times.9 In addition, HT and ischemic stroke were linked to CCA IMT thickening.8
Clinical manifestations of ICA diseases can be divided into two syndromes consisting of cerebral hemispheric infarct and ophthalmic ischemia. Brain parenchymal symptoms include motor weakness, abnormal movement, sensory disturbance, dysphasia, dysphagia, and visuospatial neglect. Ophthalmic symptoms include amaurosis fugax and visual impairment which can be temporary (retinal transient ischemic attack) or progressive to permanent visual loss with central retina occlusion.7
There are several screening and diagnostic tests including magnetic resonance angiography (MRA), computerized tomography (CT) or computerized tomography angiogram (CTA) and carotid angiography. However, the carotid duplex ultrasonography is a cost-effective tool for carotid artery disease diagnosis. The duplex examination is non- irradiating, time-saving and is accessible bedside. The carotid duplex test examines the carotid artery and vertebral artery systems which provide blood supply to both the anterior and posterior cerebral circulation. The examination can detect occlusion, stenosis, abnormal plagues in lumens of the carotid system and the IMT of arterial vessels. The IMT reflects abnormality of the arterial wall which in turn leads to subsequent stenosis or obstruction leading to inadequate blood supply to the brain.10 In the present day, carotid duplex ultrasound is a convenient procedure with high resolution and accuracy.11,12
Patients with asymptomatic CAD including atheromatous plague, thickening of the IMT or stenosis are supposed to follow recommendations for stroke prevention to reduce the risk of disease progression. HT should be controlled to remain under 140/90mmHg.13 LDL ought to be kept below 100mm/dL using statin medication12 and cessation of smoking is compulsory to reduce risk. Since carotid artery disease is a risk factor of cardiovascular disease and stroke, patients with an existing or suspected carotid artery disease should adopt lifestyle changes appropriate to both developing ischemic heart disease and stroke. This includes maintaining a healthy body mass index (BMI) in the range of 18.5-24.9 and doing enough aerobic exercise.13
Treatment is considered for symptomatic carotid patients with moderate to severe stenosis (≥ 50% stenosis) and asymptomatic stenosis with a threshold of 60%. A carotid endarterectomy may be performed to directly remove atheromatous plague to re-canalize vessel diameters. Carotid stenting may be considered as an alternative option to insert a stent to widen the arterial lumen without major surgical procedures required. Treatment options are suitable for particular conditions.14 A review of 11 studies comparing efficacy and safety between carotid endarterectomy and stenting, conducted in 4,796 patients, showed that carotid endarterectomy provided more efficacy in the short-term (a year). However, there was no significant difference between both procedures in middle-term efficacy (1 to 4 years). Conversely, carotid artery stenting provided lower rates of cranial nerve injury and myocardial infarction. Comparing endarterectomy with medication and medication alone in asymptomatic patients showed that combination therapy provided slightly more efficacy. There were less ipsilateral strokes and less intra-operative deaths than in patient’s taking medication alone (at a ratio of 5:11).15
Most studies regarding CAD have been conducted in symptomatic patients; however asymptomatic cases are vitally important since they carry a risk factor for cardiovascular disease and stroke. A comprehensive carotid research among Thai populations has not been undertaken. Once carotid arterial disease is diagnosed and recognized, clinicians can effectively provide useful interventions to patients in order to reduce subsequent comorbidities.
Research Method
The study design was a cross-sectional and observational study.
Population
The study was conducted in an asymptomatic Thai population who took an annual health check-up at the BMC during a 10 month period from June 1, 2011 to March 31, 2012. A total of 2,105 participants who had never previously experienced stroke were enrolled in the study. Patients from other ethnic groups, and patients with established CAD such as amaurosis fugax, transient ischemic attack or unknown cause drop attack and a history of stroke were excluded from the study.
Data collection
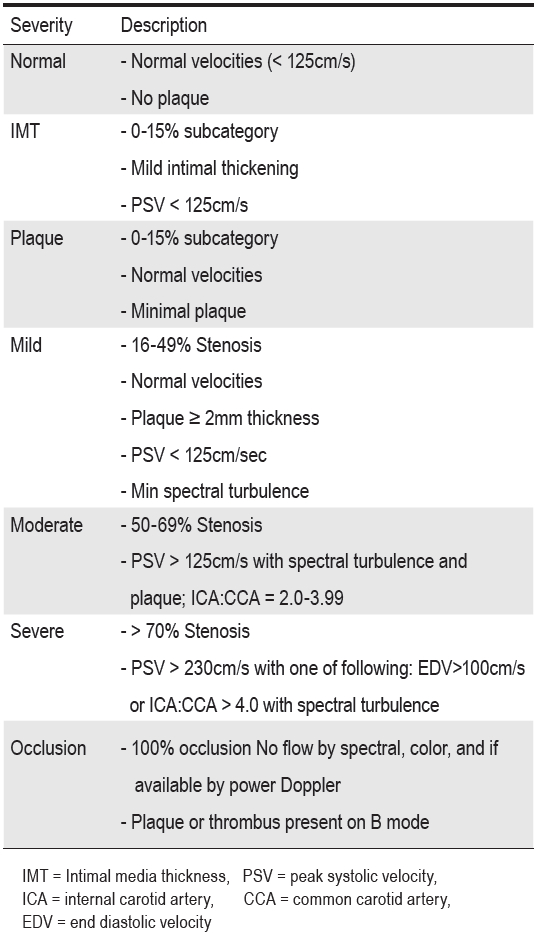
Enrolled participants were examined for CAD by experienced sonographers with two-dimenstional (2-D), colour-mode and pulse-wave doppler ultrasonography together with a standard procedure. The off-line results were completely interpreted following standard criteria.16 Demographic data were collected including age, gender, exercise activity, smoking and drinking status. Comorbid diseases including DM and HT were also recorded. Body and biochemical profiles were measured, blood pressure, BMI, fasting plasma glucose (FPG) and lipid profile (total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL) and triglyceride (TG)). Carotid duplex examinations were categorised into normal and abnormal results. Abnormal results were classified according to the severity category following the consensus criteria for carotid stenosis into plaque of the Society of Radiologists, the thickening of the IMT, and stenosis (mild, moderate and severe) (Table1).
Data Analysis: SPSS (Statistical Package for Social Science) version 19.0
1. Demographic data including gender, age, carotid results and risk factors were presented by descriptive analysis of frequency, percentage, mean, and standard deviation.
2. Risk factors for contributing abnormal carotid artery were analyzed using a multiple logistic regression method and risk was also reported as a prevalence rate ratio.
Table 1: Degrees of Carotid Artery Stenosis.16
Demographic data
The majority of enrolled participants were between 40-59 years of age with the mean of 54.1 ± 10.4 SD and ages ranged between 25 and 89 years old. Male and female patients were approximately balanced proportionally (50.8% & 49.2%). Most participants had a normal BMI but 24.2% (around a fourth) fell into the overweight category (Table 2).
Over half of participants did not smoke while 44.6% were active smokers, and 6.3% of subjects were regular drinkers whereas most subjects (61.7%) did not consume alcohol. About 42.2% of subjects occasionally exercised and 45.8% performed regular exercise (Table 6). Approximately 30.5 % of subjects had HT and 9.3% of them were diabetic (Table 3).
Carotid study results
A total of 2,105 participants underwent a carotid duplex examination, 912 cases were found to have an abnormal carotid artery accounting for a prevalence of 45.7%. Degrees of abnormal severity are classified in Table 4 below. Plaque was found in 784 cases (37.2% of participants) and the frequency of IMT thickness was 14.9% (314 cases). ICA stenosis was reported, including mild stenosis, in 11 cases, moderate in 9 cases and severe in 2 cases but there was no occlusion observed.
There was a significantly higher prevalence of abnormal carotid arteries in the elderly, in males, and in patients with higher BMI, who are smoking and drinking alcohol (p < 0.05). A history of HT and DM were also statically different in the prevalence of abnormal results (Table 3 and 5).
Body and biochemical profiles
Blood pressure ranged within normal levels for 18.3% of subjects. 19.1% of participants had pre-hypertension and 27.7% had grade-I HT. There was a significant difference in the prevalence of an abnormal carotid study among those with higher degrees of blood pressure. Thirty six percent of subjects were found to have a FPG of more than 100 mg/d and there was a higher prevalence of abnormal carotid studies in the higher FPG group (Table 4).
In the lipid profile study, those who had high levels of LDL, cholesterol and TG were 54.6%, 59.8% and 25.3% respectively. There was no association between TG, cholesterol, and HDL levels in males with carotid abnormality but lower HDL levels in women was statis-tically associated to abnormal carotid results (p = 0.02).
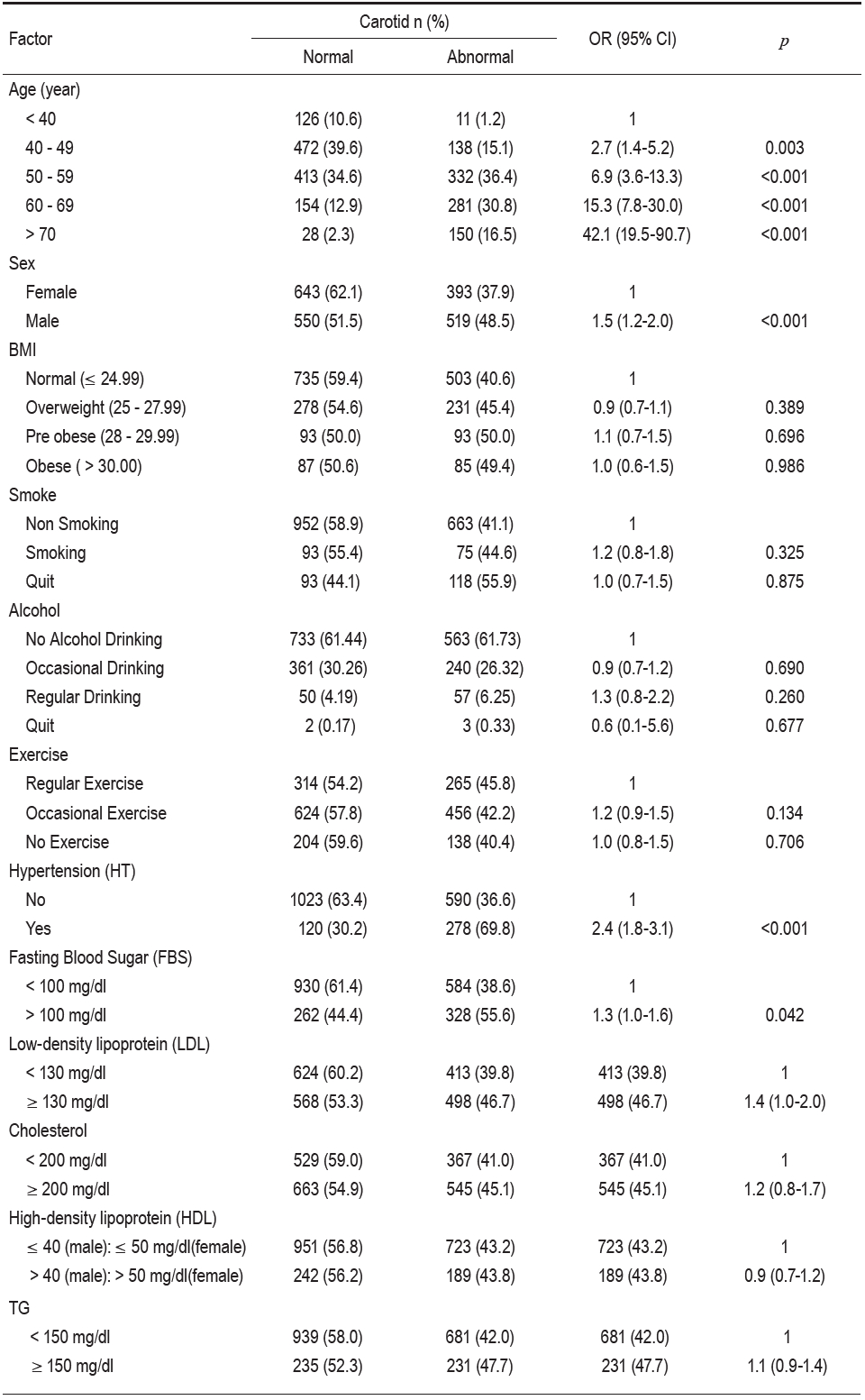
Risks for acquiring an abnormal carotid study (Table 6)
Using logistic regression analysis showed risks factors for acquiring abnormal results. Age was an independent factor and a dose-response trend was observed from the analysis. Patients aged under 40 were classified as a reference and increasing age was found to be a risk factor to identifying carotid abnormality (p < 0.001).
Male patients were 1.5 times more likely to have an abnormal carotid study (95% CI 1.2-2.0). HT associated with carotid abnormality (OR 2.4, 95% CI 1.8-3.1) whereas BMI, smoking, alcohol drinking and exercise status was not significantly linked to abnormal results.
For the biochemical profile, the relative risk of having FPG ≥ 100mg/dL and LDL ≥ 130mg/dL for acquiring an abnormal carotid examination were 1.3 (95% CI,1.0-1.6) and 1.4 (95% CI,1.0-2.0) respectively. Higher HDL level also showed a protective effect against abnormal carotid duplex, but it was not statistically significant (0.7-1.2, 95% CI).
Table 2: Patient characteristics.
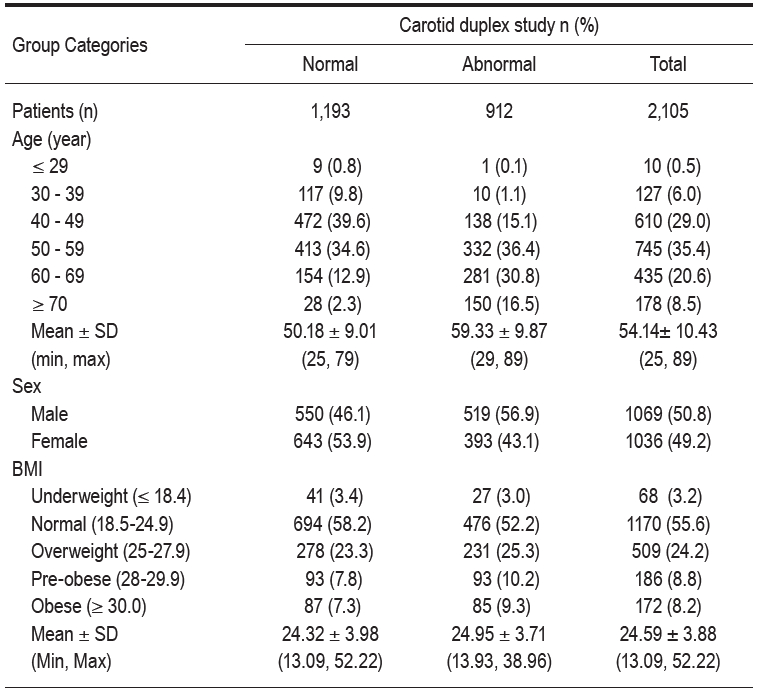
Table 3: Correlation between underlying diseases and carotid results.
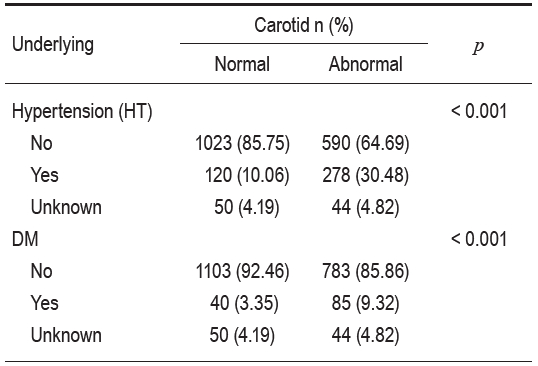
Table 4: Classification of the severity of abnormal carotid artery. (n = 2,105).
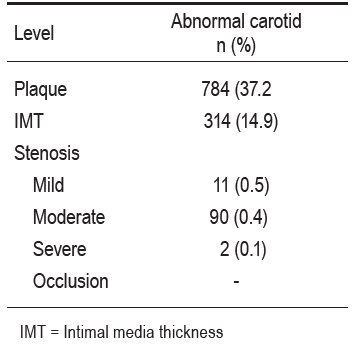
Table 5: Correlation between blood pressure (BP), Lab results and carotid duplex results.
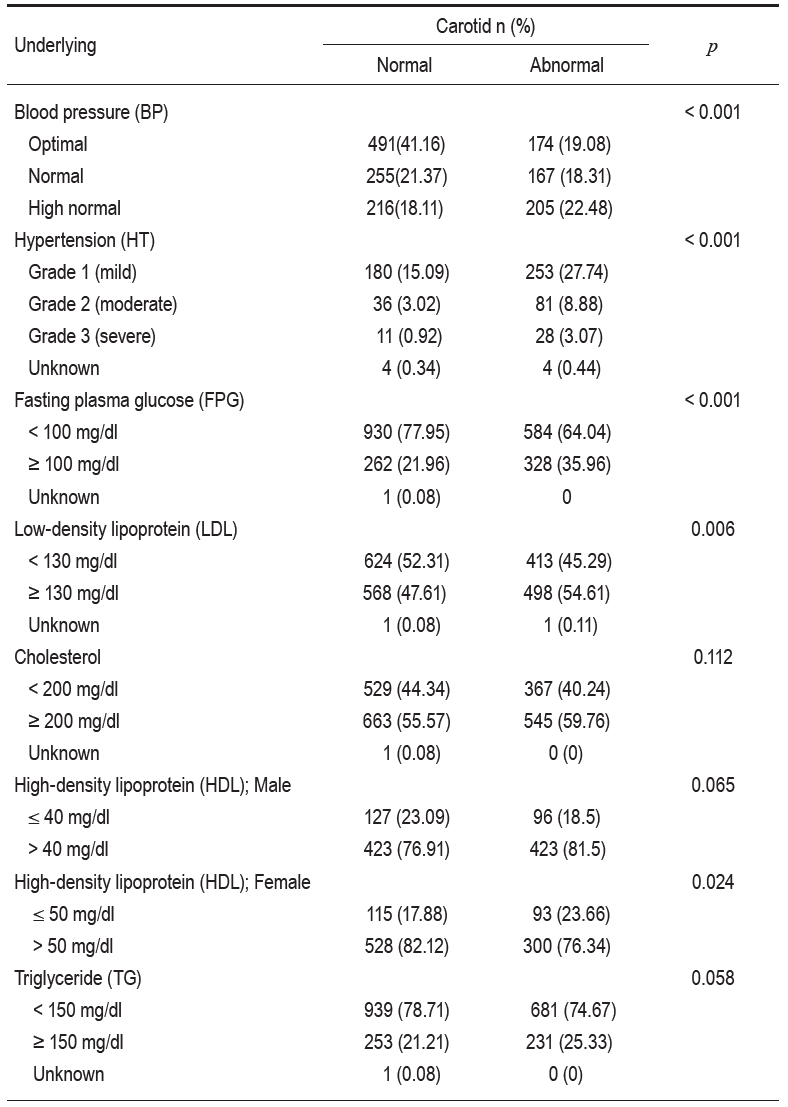
Table 6: Factors related to the carotid duplex results analyzed by multiple logistic regressions.
Carotid atherosclerotic disease is common in patients with ischemic stroke and transient ischemic attack accounting for 4-12% of cases. The prevalence of asymp-tomatic carotid stenosis in developed countries was 2-8% in people with risk factors and they were twice as likely to develop acute ischemic stroke.17
A study performed in Thailand showed that acute cerebral ischemia was caused by ICA stenosis in approximately 4-5% of cases.6 Asymptomatic carotid stenosis is an important disease that may cause stroke or can be an indicator for other atherosclerosis. Carotid disease is a marker for comorbid poly-vascular diseases, for instance coronary artery disease and peripheral artery disease. The American College of Cardiology recommended carotid endarterectomy and alternative stenting in asymptomatic carotid stenosis of 80% either prior to or combined with coronary artery bypass surgery.18
The annual rate of ipsilateral stroke associated with asymptomatic carotid stenosis is 2-4% and risk can be reduced to <1% by medical therapy. Although guidelines in management of carotid stenosis are marginally different between countries, risk factors modification and antiplatelet are commonly recommended.19 Carotid revascularizations in asymptomatic stenosis including endarterectomy and stenting are advised in several circumstances.20
This study is a hospital-based cross-sectional study and aims to identify concealed carotid disease in the general population. These results may not represent the prevalence in the community, however, the number of enrolled participants in this study is sizable and sufficient to characterize carotid issues experienced in Thai populations who have never previously experienced cerebro- vascular disease. The study showed that the prevalence of asymptomatic carotid abnormalities examined by a carotid duplex scan was 45% and the abnormalities consist of stenosis 1%, plaques 37.2% and thickening of the IMT 14.9% of total participants. Interestingly, abnormal carotid examinations were identified in young people (49 year olds and younger), which suggests that active atherosclerotic disease can develop at a younger age. High BP, FPG, and LDL on the examination day, indicating poor control of risk factors, were linked to abnormal duplex findings.
The high prevalence of abnormal carotid duplex ultrasonography in asymptomatic Thai middle-age populations, with or without risks of stroke, reflects the high magnitude of extracranial atherosclerosis. The significance of risk factors including age, gender (male), DM, hypercholesterolemia and HT correlated with the carotid artery abnormalities.
A regular carotid duplex check-up would, at least, be helpful to identify people at risk and encourage people to be concerned with their cerebrovascular risks. In spite of the fact that subjects may not require surgical or endovascular stenting for stenosis, atherosclerotic pathology of the carotid artery including plaques and thickening of the IMT will alert them to their cerebro- vascular risks and also other co-existing vascular disease. Information obtained from the carotid duplex examination has provided participants with information to help control risk factors and to improve their awareness of cerebro- vascular disease. Combined with clinical data, the carotid duplex ultrasonography provides useful information, as a preventive program for stroke and poly-vascular disease, and in appropriate situations the duplex scan should be incorporated.
The abnormal carotid arteries that were detected by the carotid duplex examinations were prevalent (approximately 45%) among asymptomatic populations who took an annual health check at the BMC. Athero- sclerotic plaque is the most common finding and significant (moderate to severe) ICA stenosis was found in 0.5% of participants. Factors including age, gender (male), DM, and HT are associated with atherosclerotic carotid disease. High plasma glucose and LDL are linked to abnormal carotid duplex scans. Early control of risk factors will reduce atherosclerotic carotid disease and delay the progression of carotid atherosclerosis.









