Electronic ISSN 2287-0237
Family is a crucial support system for all family members, especially when faced with chronic illnesses including thalassemia.1 Thalassemia is an inherited disease that requires continuous care. The standard treatments for children living with thalassemia are folic acid supplements, blood transfusion, iron chelation therapy, and splenectomy or stem cell transplantation in selected cases. Children living with thalassemia inevitably encounter the immense impacts of this inherited disease and its treatment, as well as needing to continue receiving care from their parents throughout their life. This situation seems likely to be the challenge event that triggers the adaptation of the entire family to meet the increased demand and the complex need of children living with thalassemia.2 The goal for caring for children living with thalassemia focuses on the children adapting well to their illness, and to be fulfilled with the feeling of responsiveness from their family to allow them to meet their developmental needs as much as possible. However, this depends upon the limitations of thalassemia. This reflects the necessity of family functioning at a high level as an important mechanism to drive family tasks to reach those goals. Family functioning refers to the capability of the whole family to maintain the function of the entire family, consisting of problem-solving, communication, role, affective involvement, affective responsiveness, and behavior control in order to provide a setting for the social, psychological, and biological development and maintenance of family members.3 In other words, family functioning shows the adaptive ability of the whole family in terms of how the family manages the care of children living with thalassemia and the extent to which they are able to incorporate thalassemia into their daily lifes.3,4 By achieving a high level of family functioning, this will result in the family providing the best care for children living with thalassemia resulting in a healthy well-being for children.5 However, there is widespread recognition that caring for children living with thalassemia in the family setting can produce a high intensity of stress and severe psychological impacts on family members which can in turn lead to disruptions in family functioning.1,5,6
From reviews, only two existing studies were found which helped to fully understand family functioning with children affected by thalassemia.3,7 Most studies were qualitative studies describing the experience of parents who have children with thalassemia.8-10 The study of the pathology and family functioning in the context of pediatric chronic conditions are well documented. The research findings showed that 13-36% of the families experienced an unhealthy level of family functioning, which reflected impairment in all components of family functioning. On the other hand, one study in Thailand7 revealed that family functioning in families caring for children with thalassemia did not differ significantly from the control group. Interestingly, the contradiction of research results between Western families and Asian families may be due to several factors that have influenced family functioning in families of children affected by thalassemia.
To precisely understand how to enhance family functioning or what strategies to promote for family functioning, the factors related to it must be answered. A greater understanding of the factors will help healthcare providers to tailor the de- velopment of effective interventions to either promote positive factors or to lessen negative factors in order to achieve a high level of family functioning in the affected families.
The aim of this study is to synthesize factors related to family functioning in the families caring for children living with thalassemia.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)11 and Joanna Briggs Institute (JBI) methods were drawn upon in the collection, study selection and critical appraisal to ensure the quality of selected studies before proceeding to the next step of articles analysis.12
The PRISMA statement13 was used as the evidence-based guidelines for conducting this integrative review. CINAHL, SCOPUS, PubMed, and PsycINFO were searched from January 1st, 2008 until October 31st, 2019. The used keywords were ‘predictive factors’ AND ‘family adaptation’ AND ‘children with thalassemia’ AND ‘family functioning’ AND ‘factor’ AND ‘family’ AND ‘stress’ AND ‘children’ AND ‘thalassemia’AND ‘chronic illness’AND ‘family well-being’ AND ‘family coping’.
The search was limited to any peer-reviewed study published in English between January 2008 and October 2019 and was included for review in order to capture all recent evidence. Journal articles were included in this review if they:
Criteria for exclusion were written in a language other than English, commentaries, narrative review, full-text unavailable, editorial, no concepts relating to, and insufficient information for critical appraisal.
After the articles were retrieved from the systematic search, these articles were evaluated by using the PRISMA 2009 flow diagram. The titles of the published articles were analyzed to determine whether most articles met the inclusion criteria or not. Next, all abstracts were evaluated, as well as the full text of those that met the inclusion criteria and presented original research on the topic were gathered and evaluated. Then, the eligible studies were included in the review through data extraction into evidence tables. The reference lists of all pertinent papers were cross-checked to ensure that no pertinent study was left unexamined.
Search Results
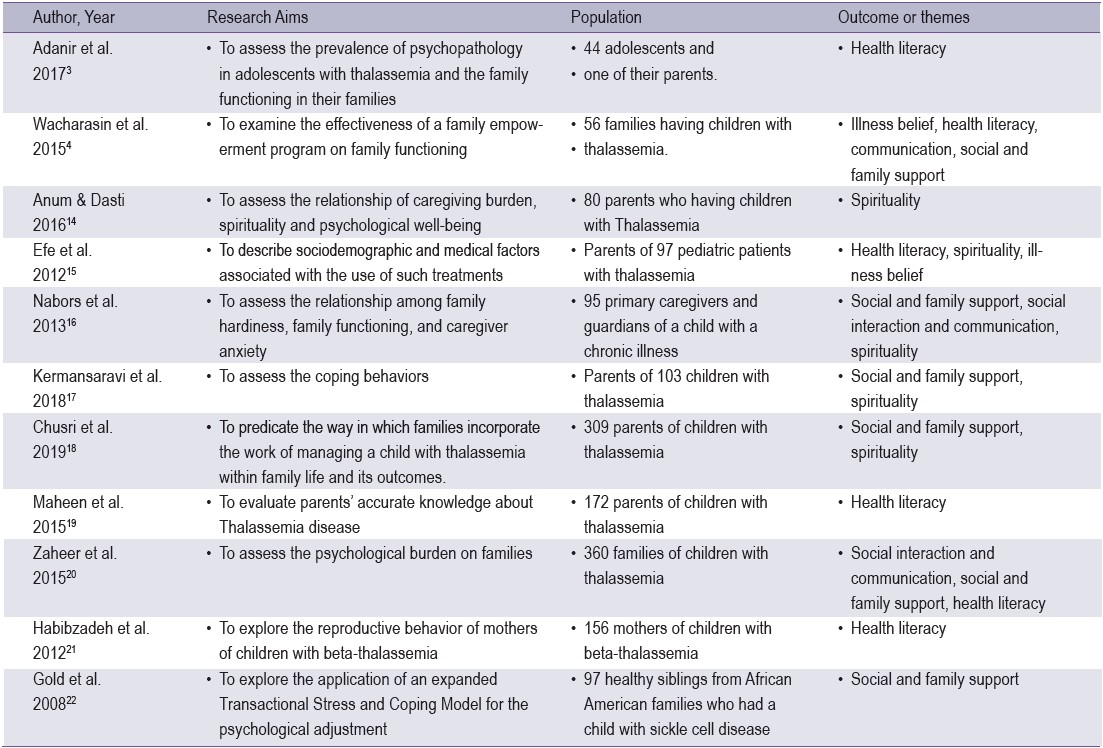
As noted above, 11 studies were included in this review from 57 reviewed full-texts and 1,354 search results. The final 11 articles were subsequently included in the review. All the eligible articles were quantitative studies. Most of the quantitative studies were correlation studies and cross-sectionalstudies (each type n = 4). Of the 11 articles, 8 were conducted in the Middle East region, 2 in Asia and 1 in Western countries. As such, the findings from the studies were presented as a narrative summary under five core themes: illness belief, health literacy, social interaction and communication, social and family support, and spirituality.
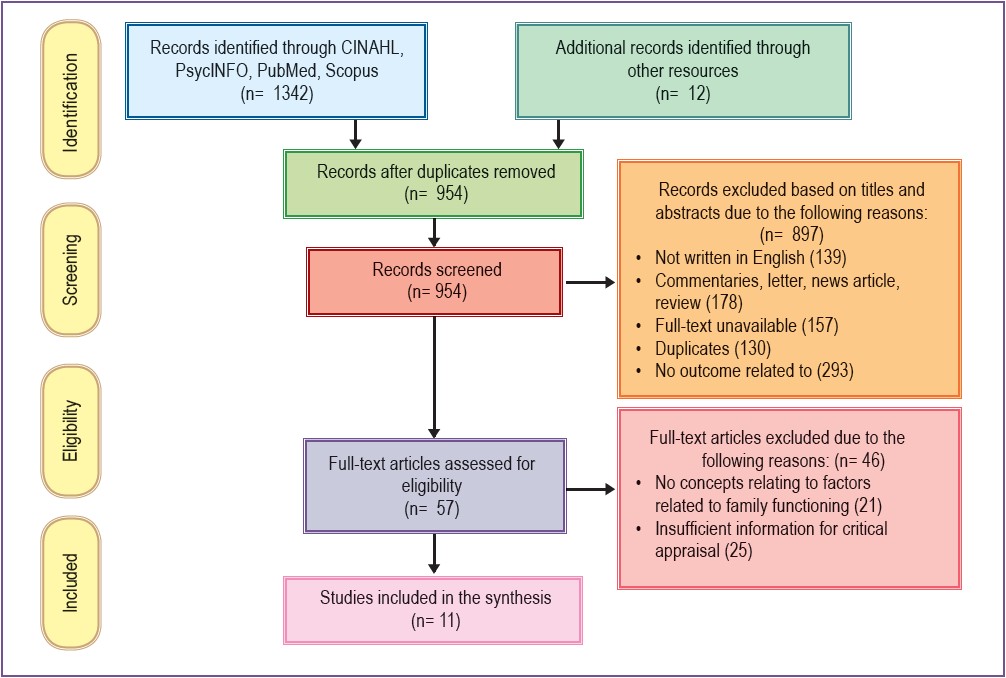
Figure 1: PRISMA flow diagram on the outcomes of search strategies.
Table 1: Studies included from systematic searches
Spirituality
Spirituality was defined as an effective natural coping resource that can help a person in times of distress. It can also be applied as a therapeutic strategy to alleviate the burden, anxiety, stress, depression, and other impacts that were inter-related. The study by Anum & Dasti,14 showed that the role of spirituality upon the psychological well-being of family caregivers, prevented pathological influences of family caregiver burden and enhanced psychological well-being by spiritual counseling. This was similar to a study by Efe et al.15 where they found that 61.8 % of the parents used prayer/spiritual practice as a kind of complementary and alternative medicine (CAM) for caring for their child. The important reason why they used CAM is because they believed this could help their children feel better. Even though the parents knew that prayer might not cure the children’s disease, it gave the family an enhanced feeling of peacefulness, where everything possible was being done for their children with thalassemia. Also similarly, a study by Nabors et al.16 found that the most common factor related to families coping was faith or religion. Prayers was perceived by caregivers as a strategy to express emotions, feelings and support for expressing their hopes and wishes for their child. The same is true in the study by Kermansaravi et al.,17 which found that parents of the children with thalassemia used coping behaviors by turning to God since this can strengthen the feeling of mental stability.
Illness belief
The study by Wacharasin et al.4 found that illness belief was a cognitive map guiding the decision when families confront a chronic situation. Illness belief was, therefore, the dominant factor that influenced family functioning and is a crucial factor to understand how families cope with illness and suffering. The study by Efe et al.15 found that 82.5% of fami- lies reported using one or more of the CAM methods as an alternative care for children with thalassemia. In this regard, nutritional supplements and animal materials were chosen as 47.4%, 35.1% respectively. The most common reason that families decided to use CAM in their children is because families perceived the helpfulness of CAM and expected that CAM could maintain their hope about their children’s illness. This especially applies in cases where the prognosis of thalas- semia worsens, because families believe that CAM will help to promote children’s health and protect them from the severe impacts of illness.
Health literacy
The study by Maheen et al.19 revealed that parents (40%) showed lower scores of knowledge about thalassemia, especially in Siraiki and the Pathans respondents (17.9 ± 4.48; 17.2±4.34) respectively. The study suggested that health education should align with cultural and linguistic diversity, and also be provided to a level that every family member could easily access. Insufficient knowledge about thalassemia combined with a strong preference for consanguineous marriage in some ethnic groups resulted in an exponentially increased risk of thalassemia disease. Genetic counseling was, therefore, a necessary intervention to promote correct knowledge about thalassemia. Astudy by Zaheer et al.20 found that the family caregiver is worried about the illness presenting in their other children. Congruence with the study by Wacharasin et al.4 showed that the family empowerment program (FEP) had provided a process of health education and genetic counseling by the hematologist to enhance knowledge competency. This leads to the critical judgment about the reproductive behavior of the family caregiver. This is consistent with the study by Habibzadeh et al.21 which stated that the average number of children in mothers who had received genetic counseling were significantly lower than those mothers who had not received genetic counseling. However, the research results also found that the mother whose 1st or 2nd child had beta-thalassemia (n = 82) had an average total number of 3.12 (S.D 1.88) children; for those whose first affected child was either the 3rd or 4th child (n = 38). This reflected the reproductive compensation in families until the family had enough boys. Importantly, the study by Efe et al.15 revealed that the physician was a key person who provided health education to promote adequate knowledge or correct concepts about thalassemia, in addition to the family elder in the context they live.
The study by Nabors et al.,16 found that difficult interaction and communication with healthcare providers was a negative factor that produced huge stress for families. Lack of communication skills, which may negatively affect their interactions with the physician or other healthcare providers, was also an important factor affecting the feeling of conflict and feeling of helplessness due to not being able to understand how to care for their child. The same is true in the study by Wacharasin et al.,4 that found that communication was a crucial step of the FEP process to enhance family functioning. In this program, the family member was challenged by the program through role-playing to talk to the physician about the children’s illness and their treatment in order to strengthen effective communicating skills. Moreover, the study found that the family caregivers who participated in the FEP learnt how to communicate with the physician and had appropriate family conversations without criticizing within the family, which helped to enhance family functioning. In addition, the study by Zaheer et al.20 revealed that families living with children with thalassemia suffered from social interaction problems caused by misconceptions about the cause of thalassemia. For example, thalassemia was thought to have been caused by the family’s sinfulness, or as a punishment from God. This illustrated that families have been stigmatized due to their children being diagnosed with thalassemia. This impacted some families, who had to confront the limitation to access adequate health care options, especially families who live in rural areas.
Social and Family support
The study by Nabors et al.16 revealed that social and family support was an important factor that helped family caregivers to cope with a chronic situation. Support can come from family and friends, relatives, neighbors, as well as assistance from healthcare providers at the local children’s hospital. The same is true in the study by Gold et al.,22 that found that family adaptive processes predicted as much as 21% of the unique variance in sibling adjustment of children with sickle cell disease. Specifically, families who endorsed high levels of family coping, support and expressiveness, and low levels of conflict, were associated with positive sibling adjustment. Congruence with the study by Zaheer et al.20 revealed that parents (58%) claimed that they trusted their spouse when they needed help and could discuss their problems to relieve themselves from the psychological burden caused by living with children with thalassemia. This was similar to a study by Chusri et al.,18 that stated that parents of children with thalassemia perceived positive outcomes after receiving support from family and from kinship. Congruent with the study by Wacharasin et al.,4 FEP had provided a process of commending abilities of family members, in the circumstance of taking care of their child in an adversarial situation, to manage and to take decisions. This program helped family members to create a family network with other families who had faced a similar situation. Family members felt an emotional support from their social support network. Also, the study by Kermansaravi et al.17 found that approximately 70.9 % of the parents in the study tried to talk to other people or other families who were in a similar situation.
The synthesis results identified five themes including: spirituality, illness belief, health literacy, social interaction and communication, social and family support. This is discussed in detail below.
Spirituality: spirituality establishes an essential cognitive assessment as a handling mechanism for the family, empowering family members to appraise negative events differently and to experience a stronger sense of control.23 Moreover, spirituality is synonymous with generosity, family members can develop self-sacrificing and altruistic feelings, which will in turn lessen their burden and enhance resilience positively affecting family functioning.14 In addition, spirituality still facilitates the feeling of fulfillment with social and family support through the process of communication.4 For example, it can help to fulfill or maintain hope for the family, encouraging family members to express feelings and emotions, active listening and positive thinking. Also, it can promote empathic relationships towards each other such as comforting family members, showing them attention and care, openness to the family member’s attitudes and feelings, and honoring them.4,14,24 The same is true in the study by Chaiyasit et al.,24 that found that people living with HIV/AIDS perceived the role of spirituality as enhancing the feeling of peace and happiness, inner strength, self-acceptance and understanding of illness, promoting self-care, increasing a sense of compassion, maintaining hope and giving meaning to their lives. This reflects a spiritual anchor to help the family maintain and improve their family functioning to transcend the difficult time of living with children with thalassemia. Congruent with the study by Chusri et al.,18 family life difficulty could explain only 2 % of the variance of family functioning. These results can be explained by virtue that the parents in this study were Buddhists who believe in karma and in a previous existence. The laws of karma teach them that if they do good, they will experience good and if they do evil, they will experience evil. This perception influences the feeling of trust in a higher power and this feels more comfortable since the family believes that everything that happens and will happen in the future has already been determined by supernatural power or belief in religion they respect.24
Illness belief: Illness belief has been instituted over a long time through the inter communication within a family by the family elders’ teaching. 25 This means it has been deeply rooted and often constitutes the basis dividual’s identity. Once the family has children with thalassemia, they are inevitably triggered to find out the best way to handle this adverse situation caused by living with children with thalassemia. The reason why they do this is because they wish to uphold their role as a natural support for the thalassemia child and all family members. Those ways have been determined based on their illness belief. Illness belief is a stage of searching realities and exploring hope and beliefs about illness. However, illness belief can be both a constraining illness belief and a resilience illness belief.25 Constraining illness belief may decrease possibilities for discoverinns and potentially increase suffering. On the other hand, resilience illness belief increases solution possibilities, diminishespan>suffering, and invites healing. Illness belief was the dominant factofluences family functioning and is a crucial factor to better understand how a family copes with illness and suffering.4,25,26 Comprehensive understanding about illness belief will help healthcares to develop interventions to enhance family functioning through promoting resilience illness belief and eliminating the constraining illness belief. Importantly, to prevent the worse impact of the prognosis of thalassemia, it is a necessity that healthcare providers should discuss and provide counseling to the family about the usefulness&nbsand limitations of those illness beliefs.4, 15
Health literacy about causes, treatments, side effects, health care guidelines for thand children with thalassemia is an important factor that helps the family receive adequate information for decision-making in order to enhance the quality of care for their child.Adequate information is the topic that healthcare providers should be concerned with to ensure whether the family receives useful and precise informm health education. If the family can receive adequate information about thalassemia, it will help them to reach an appropriate cognitive adjustment to handle the challenging situations they face in order to maintain their family functioning. For instance, genetic counseling, setting up a social media group connecting families living with children with thalassemia are a few useful channels that could act as knowledge bridges to help those families access the information at their discretion.6,27 Importantly, genetic coubsp;is a significant intervention in helping the family alleviate suffering from stigmatizatd by their communities’ misconception about tof thalassemia. Furthermore, it is very useful to prevent the reoccurrence of new patients from reproductive compensation behavior in some regions.28,29 However, even genetic counseling seems to be a significant strategy of the health care system in terms of diminishing the number of new patients, bunt ethnic groups and beliefs in their contexts are in fact vital issues that should also be determined when conducting genetic counseling.6
Social interaction and communication: this problem results from the misconceptions regarding the cause of thalassemia that are usually found more often in families living in rural areas rban areas.16,20,28,29 This problem impacts families and their children where society treats them as criminals because it is implied they are punished by divinity.<e="font-size: 6pt; vertical-align: 3pt;">6 These beliefs can cause a terrible impact for the family, either in restricting social interaction or dissatisfaction in the interaction that potentluences the occurrence of the family’s psychological suffering.18,20,26 Additionally, communication problems is a common cause that produces significant distress in families living with children with thalassemia, especia rural areas. They usually lack communication skills or do not dare to ask physicians or other professionals regarding the child’s illness.4,6 This problem impacts the family ability to access adequate information to handle adverse situations resulting eventually in the family’s failuage their family functioning adequately. Therefore, healthcare providers need to provide effective communication which encompasses all necessary topics, as well as professional gestures in the way of generosity and a humane approach. In brief, healthcare providers are key in promoting a correct understanding in this regard. This will lead to better social interaction and communication between the family, healthcare providers, and society. This will ultimately help the family to perceive and to use society at its utmost as a social support source that can certainly enhance family functioning.
Social and family support: it has been acknowledged as an important factor related to family functioning.1-5 Family must realize the importance of family relationships and societal values toward improving family functioning. Hective problem management is more subject to how families are functioning.4,5 Thai family members usually live together and spend the majority of their time at home. Additionally, the family often receives support not only from family members, and theirs, but also from neighbors to maintain care roles.14,18 In this regard, Thai family culture is influenced by Buddhist doctrines in terms of cultivating a positive attitude and expressing friendly concern towards other families. Thas, therefore, do not want other families to experience the suffering as they have encountered.4,18
The five identified themes have a close relationship to each other where, when one happens, the other may follow. All five themes, therefore, can be integrated into an effective intervention to promote family functioning in families living with children with thalassemia. Specifically, the best way in this regard, is health education by integrating these five themes as important factors to enhance family functioning. The health education may be conducted through social media groups, electronic books, booklets, hotlines, group counselling, etc. The necessary information should encompass general information about thalassemia such as definition, cause, signs and symptoms, treatments, and its impacts. The correct and adequate information will help the family to provide the best care for their child. Also, correcting misconceptions of their communities regarding the cause of thalassemia will result in improving social interaction and communication. Furthermore, effective social interaction and communication will provide the family with a way to perceive social and family support which will be useful to effectively deal with difficult times as well. In addition, communication skills are a necessity for the family to involve the physician in the caring process of their child. At the same time, the physician should provide the family with enough time and a humane approach to allow the family to receive precise adequate information and useful support from healthcare providers. Likewise, the family’s illness belief should be assessed, to determine whether it is either a constraining or resilience illness belief. For example, if they believe that thalassemia is due to the family’s sinfulness and is incurable, the family will probably ignore the call forcontinuous treatment and this will eventually produce a hazardous effect on their child. Hence, healthcare providers need to correct those constraining illness beliefs. On the other hand, resilience illness belief should be promoted such as if the family believes that because it is the family’s sinfulness, so, the family must bear the responsibility to care for their sick child. Finally, spirituality by the family’s meaning should be assessed since it is perceived as a magic source of family power that can lessen the feeling of burden caused by living with children with thalassemia, and increase a stronger sense of control to transcend difficult times. In this sense, spirituality may be religion, supernatural power, ceremony practice, generosity, or whatever they respect in order to enhance the feeling of peace and happiness, inner strength, self-acceptance and illness understanding, promote self-care, increase a sense of compassion, maintain hope and create meaning in their lives.
Significantly, the results in this study are synthesized from the studies that were conducted in different regions. This means each factor in this study should be determined for use. For example, in the middle east region, most people are Islamic and usually face challenges arranging for blood transfusions in the holy month of Ramadan, as people normally avoid blood donations at this time.20 On the other hand, this problem is not found in western and Asian countries where most people are of other religions. Likewise, health literacy regarding thalassemia is still a major problem in developing countries such as Asia and middle eastern countries.19,21 Furthermore, families living in rural areas are more distressed than families living in urban areas. Most parents have to face a lack of available blood and a lack of adequate knowledge to take care of their child, resulting in a lack of awareness to prevent the occurrence of new patients.20,21 Meanwhile, in Western countries, most people live a busy and active social life compared to rural residents.20 Such a situation is combined with most families being nuclear families (a major family type found in urban areas). It affects those people who may not have a chance to immerse themselves with effective social interaction and communication, and they may not perceive social and family support from their communities. The different cultures in each region, therefore, should be considered while planning an intervention to enhance family functioning in families living with children with thalassemia.
Family functioning is widely accepted as an important concept that has been believed to play a vital role in caring for children with chronic illnesses, including thalassemia. The family, therefore, is a powerful natural support system for children living with thalassemia and other family members. That means the quality of care provided for children with thalassemia depends on whether the family can perform their family functioning well or not. Therefore, this understanding will guide healthcare providers to integrate these factors for the development of an effective intervention to enhance family functioning in families living with children with thalassemia.









