Electronic ISSN 2287-0237
1. To quantify the value of myocardial regional wall motion and to study the inter-segmental integration pattern of the circumferential regional wall motion of the left ventricle using Magnetic Resonance Imaging (MRI) in patients with normal global and regional left ventricular systolic function (LVEF ≥ 55%) and compare results to groups with impaired left ventricular systolic function (LVEF ≤ 55%).
2. To prove that the inter-segmental integration pattern of normal myocardial regional wall motion is consistent and can be used effectively as a complimentary tool with visual estimation method to detect the impaired myocardial regional wall motion.
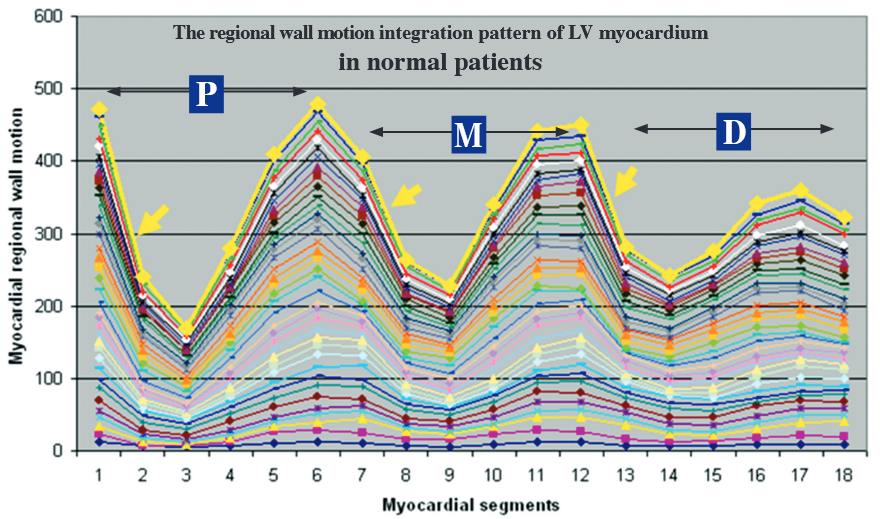
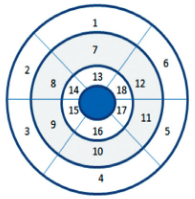
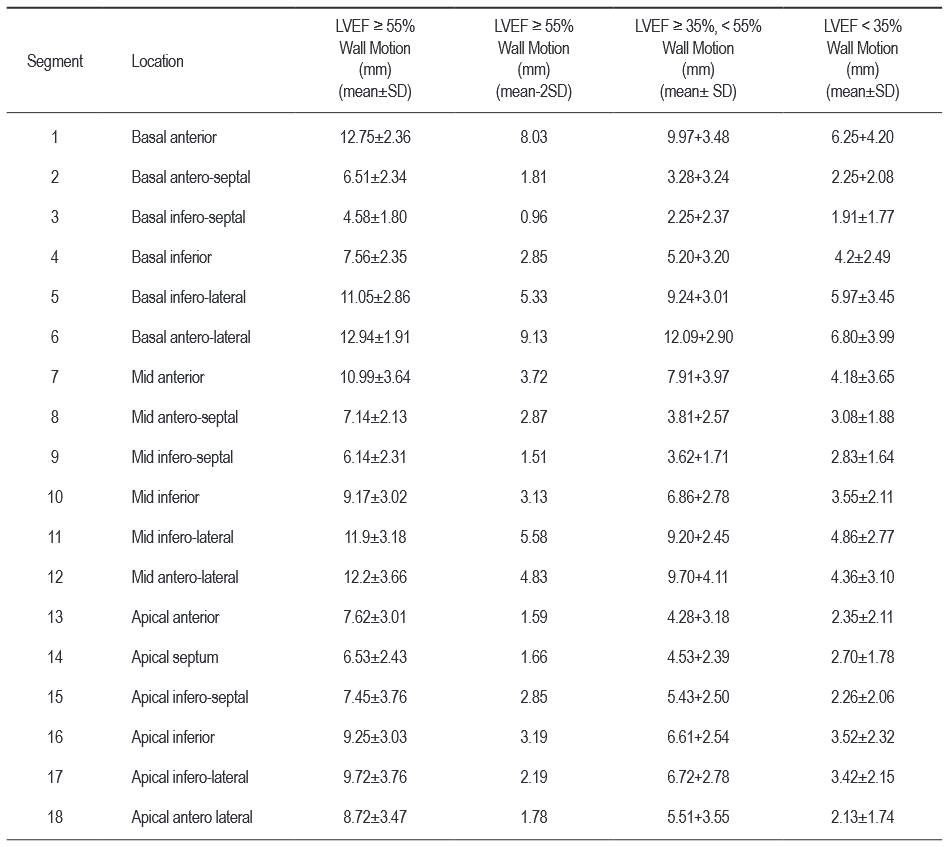
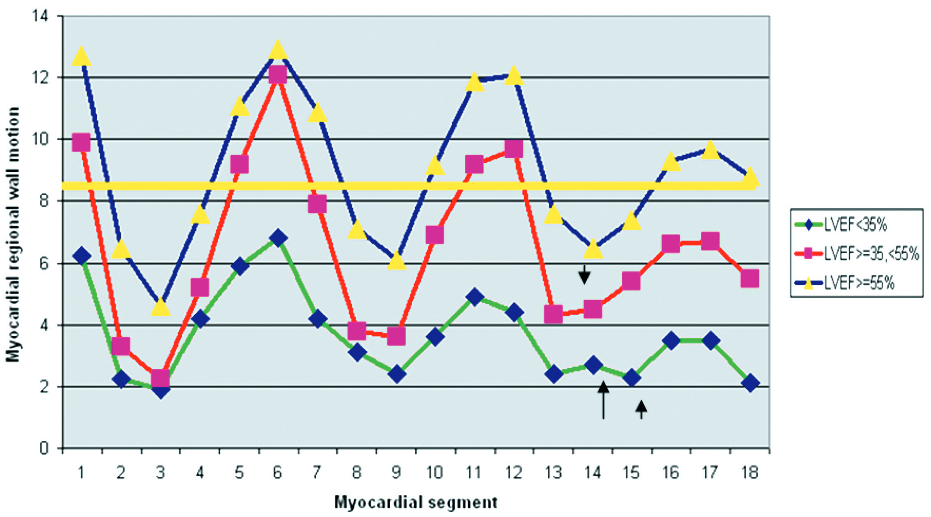
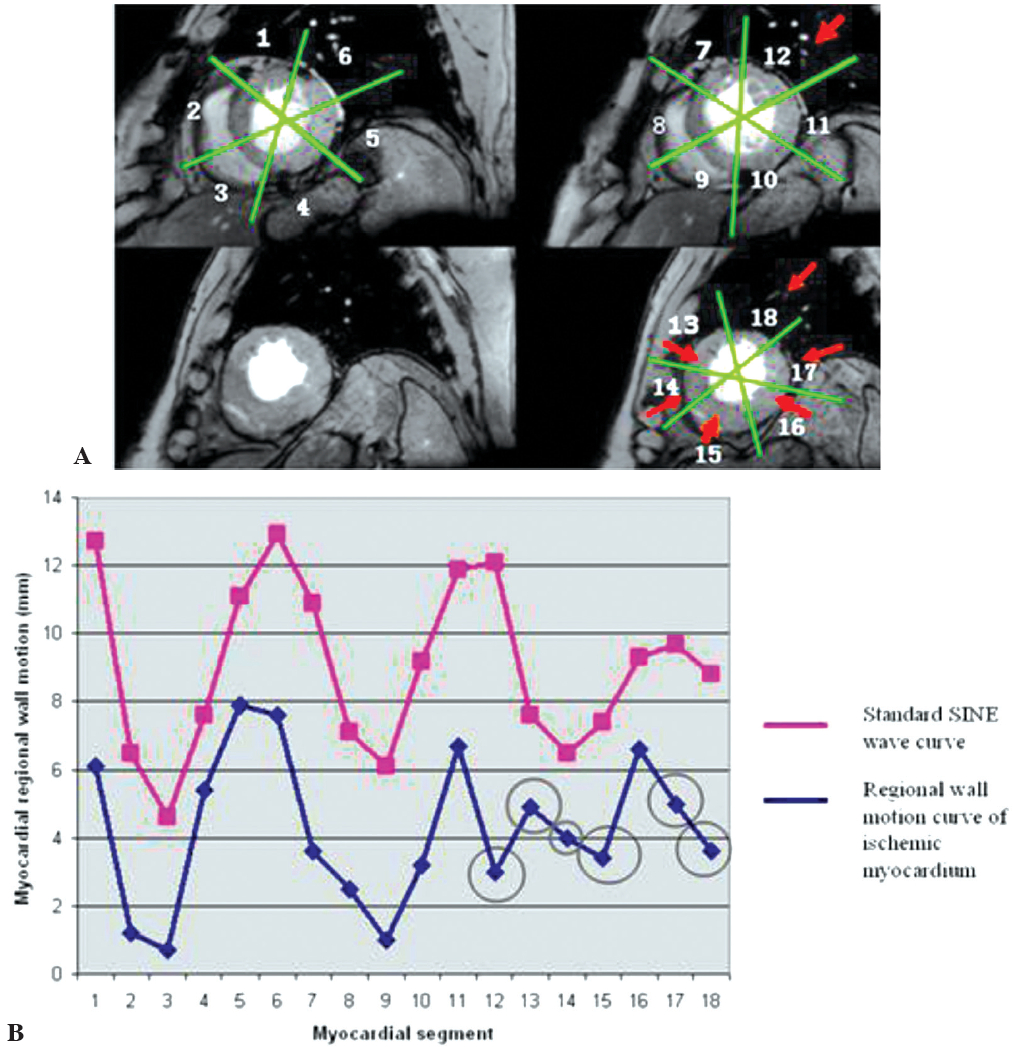
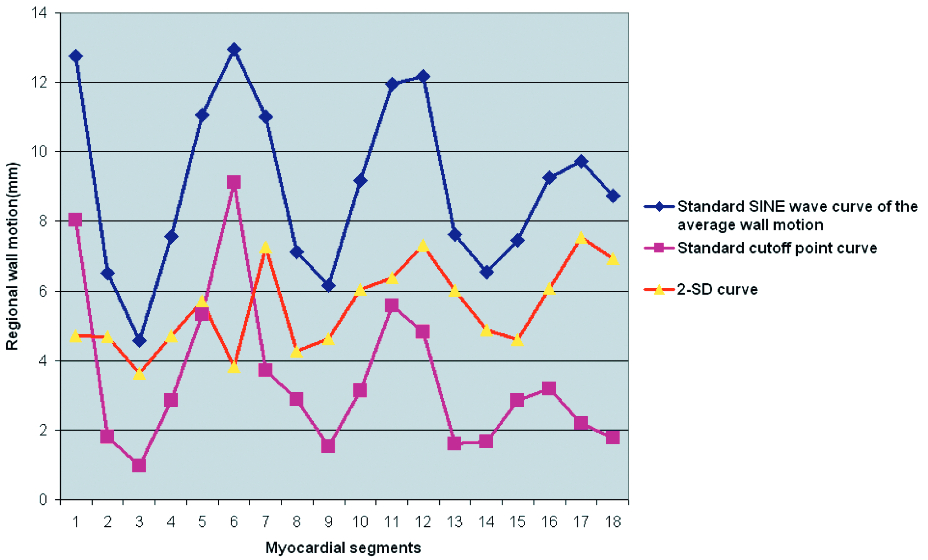
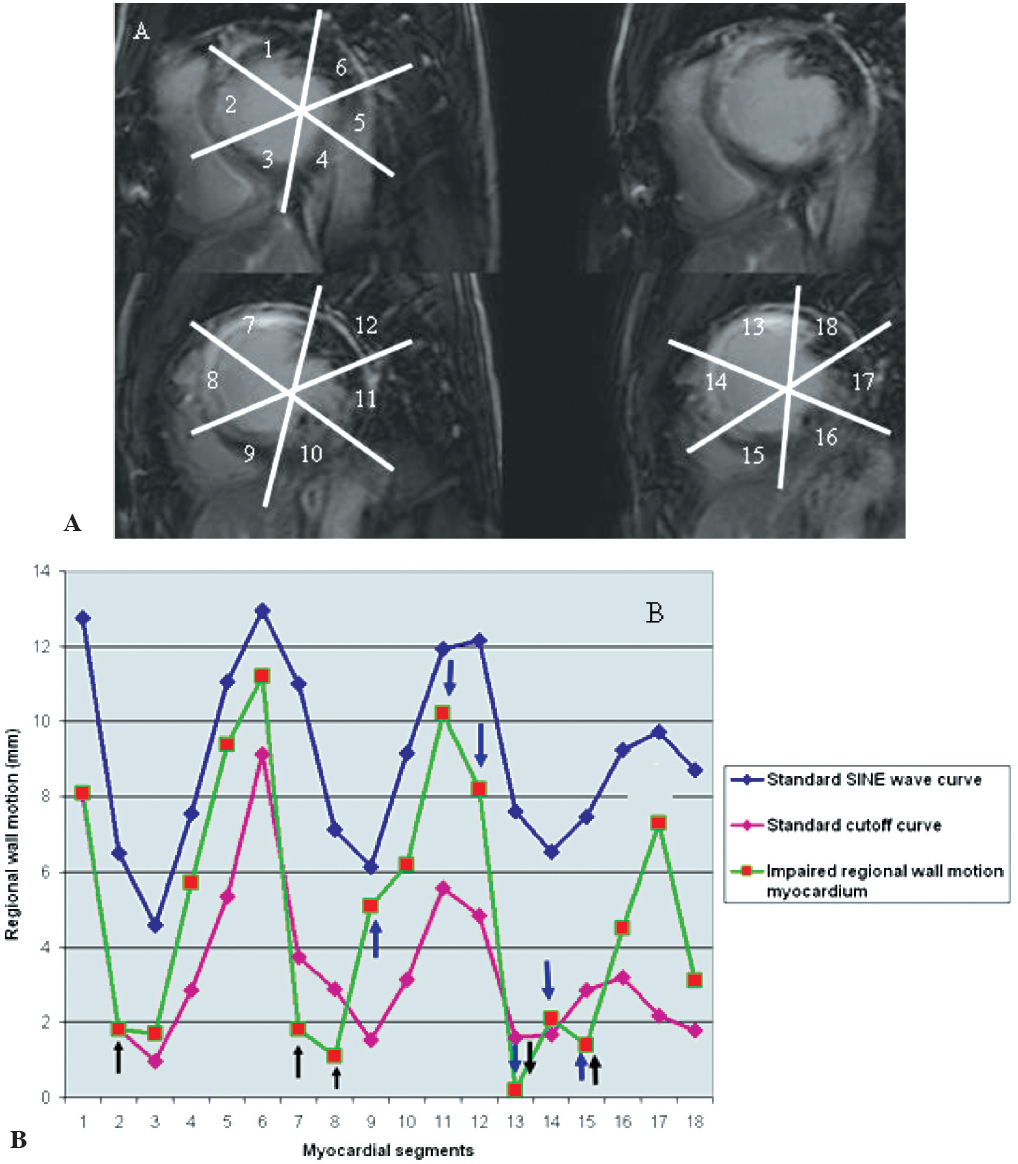
A total of 60 adult patients (above the age of 15 years old) who underwent cardiac MRI during January to October, 2011 were recruited. Thirty-six patients had normal ejection fraction (LVEF ≥ 55%, Mean = 64%) and normal myocardial regional wall motion, 12 patients had moderate systolic dysfunction (LVEF ≥ 35%, < 55%, Mean = 49.3%) and 12 patients had severe systolic dysfunction (LVEF < 35%, Mean = 22.8%). We retrospectively analyzed and measured the left ventricular ejection fraction and regional wall motion by computerized program in the Brilliance work station of 3 Tesla (3T) MRI. The myocardial wall was divided into 3 parts, the basal (the myocardial level above papillary muscle), the mid (the myocardial level at the papillary muscle) and the apical part (the myocardial level below the papillary muscle). Myocardial wall in each part was segmented into 6 segments for regional wall motion assessment, which was modified from the American Heart Association (AHA) recommendation. The regional wall motion in each ejection fraction group was measured in millimeters and averaged. The average value of each myocardial segment of each systolic function group was plotted in line curve from segments 1-18 (basal to apical part) to form the qualitative standard curve (Standard inter-segmental integration curve or Standard SINE wave curve) of normal regional wall motion. The myocardial segment specific standard deviation (SD) value of the normal cardiac function group was also calculated. We created the standard cutoff point curve by plotting the resulting value of the average regional wall motion value of each myocardial segment (1-18) minus the segment specific 2-SD of the average value of regional wall motion of the normal cardiac function in line curve. The standard cutoff point curve was a double functional tool because it both displayed SINE wave curve character and provided quantitative cutoff point value. We used the standard cutoff point curve in combination with the standard SINE wave curve to detect impaired myocardial regional wall motion. The impaired regional wall motion myocardial segment was considered as a distortion or deviation point from SINE wave and/or the point of curve that stood below the cutoff point value. The accuracy of these tools indetecting impaired myocardial regional wall motion were compared to visual estimation in terms of sensitivity, specificity, positive predictive value and negative predictive value.
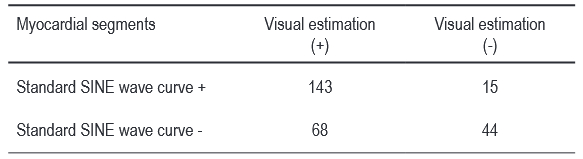
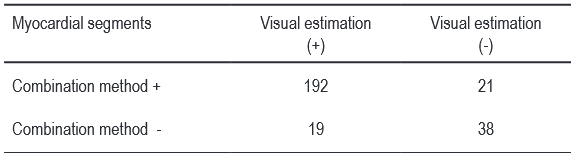
By comparison to the visual estimation method, the sensitivity, specificity, the positive predictive value and the negative predictive value of the standard SINE wave curve in impaired myocardial regional wall motion detection were of 67.8%, 74.6%, 90.5% and 32.2% respectively. By combining the standard SINE wave curve with the standard cutoff point (mean value - < 2-SD) curve to detect impaired myocardial regional wall motion, the sensitivity, the positive predictive value and the negative predictive value were increased to 90.9%, 90.4% and 66.7% respectively, compared to the visual estimation method.
The circumferential regional wall motion integration pattern of the left ventricle in normal LVEF with normal regional wall motion patients is consistent; if characterized as a SINE wave curve, it can be used in combination with the standard cutoff point curve which displays the SINE wave character with a quantitative cutoff point, thus providing us with an additional support tool, to the visual estimation method, to detect impaired myocardial regional wall motion with acceptable high accuracy.
MRI, Gradient echo CINE MRI, Standard SINE wave curve, Standard cutoff point curve (mean- 2SD)
10.31524/bkkmedj.2012.02.004