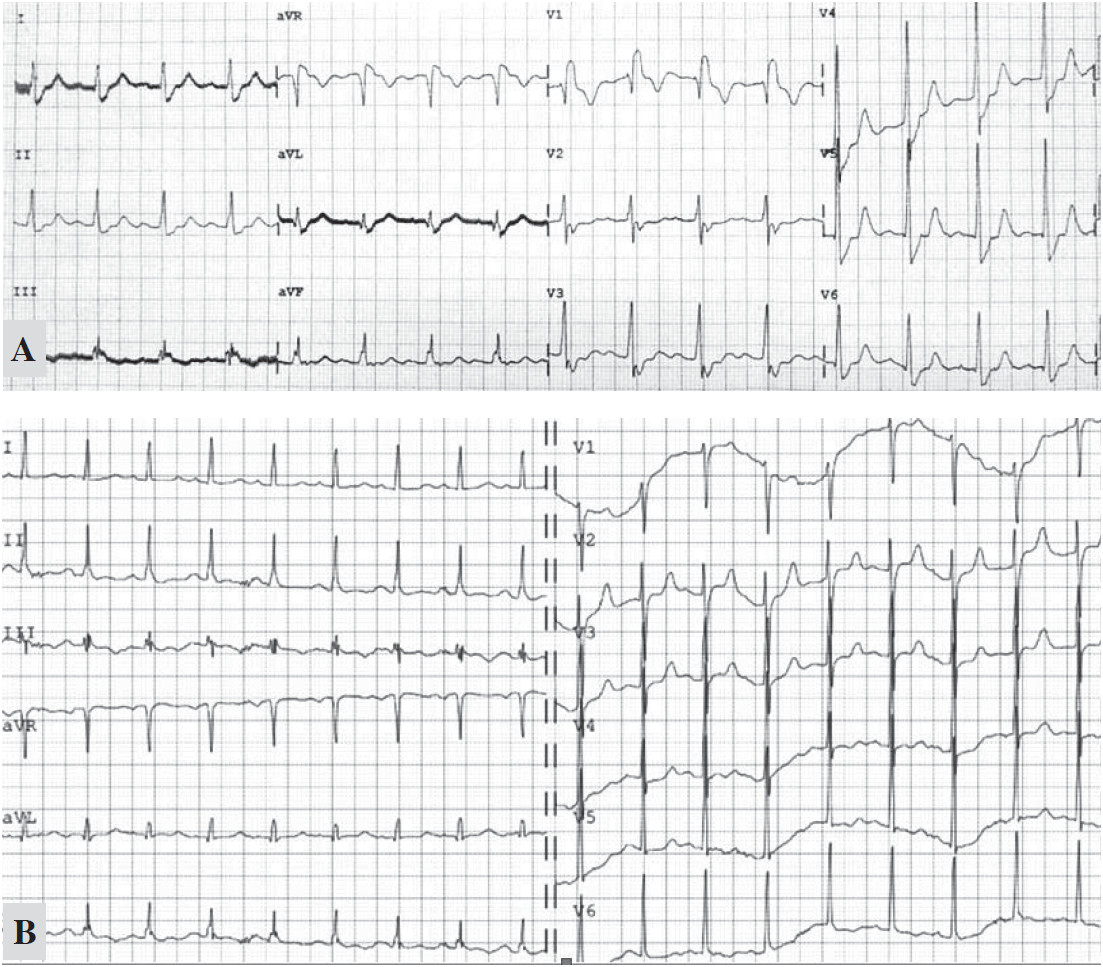
1A: Post-arrest ECG showed a sinus rhythm rate of 100/min, complete RBBB, J point ST depression in V2-4, ST elevation in leads aVR and lead III. 1B: the RBBB pattern disappeared on the following day.
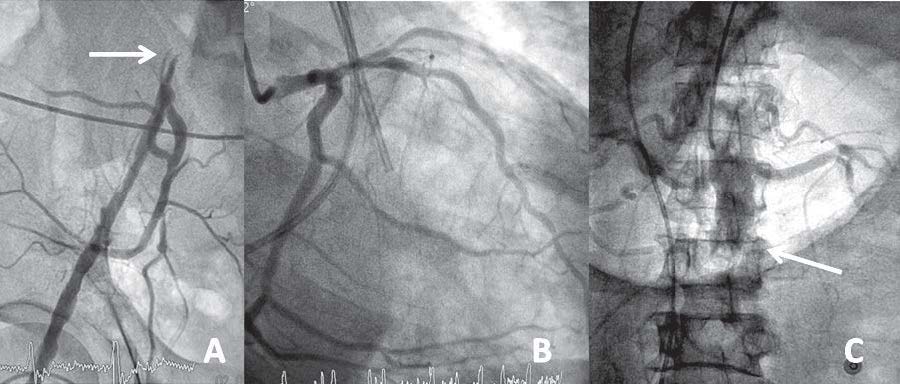
Figure 2:
An occluded iliac artery (A), non-obstructive left dominant coronary angiogram (B) and occluded infra-renal aorta (C).
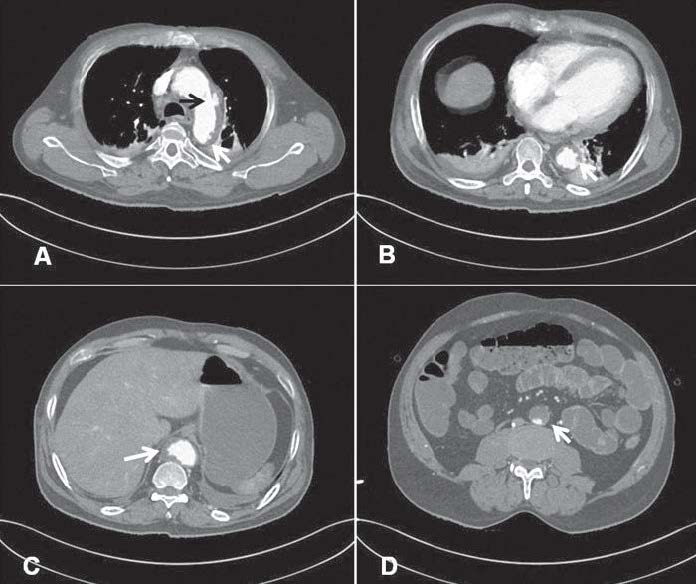
Figure 3:
CT shows a large penetrating aortic ulcer (PAU) at the lateral wall of the aortic arch (A, black arrow), multiple small PAU along the abdominal aorta with intramural and mural thrombus (white arrow, A-C). The inferior renal abdominal aorta is occluded with thrombus. Bilateral pleural effusion and atelectasis are also noted (Figure 3A-B).
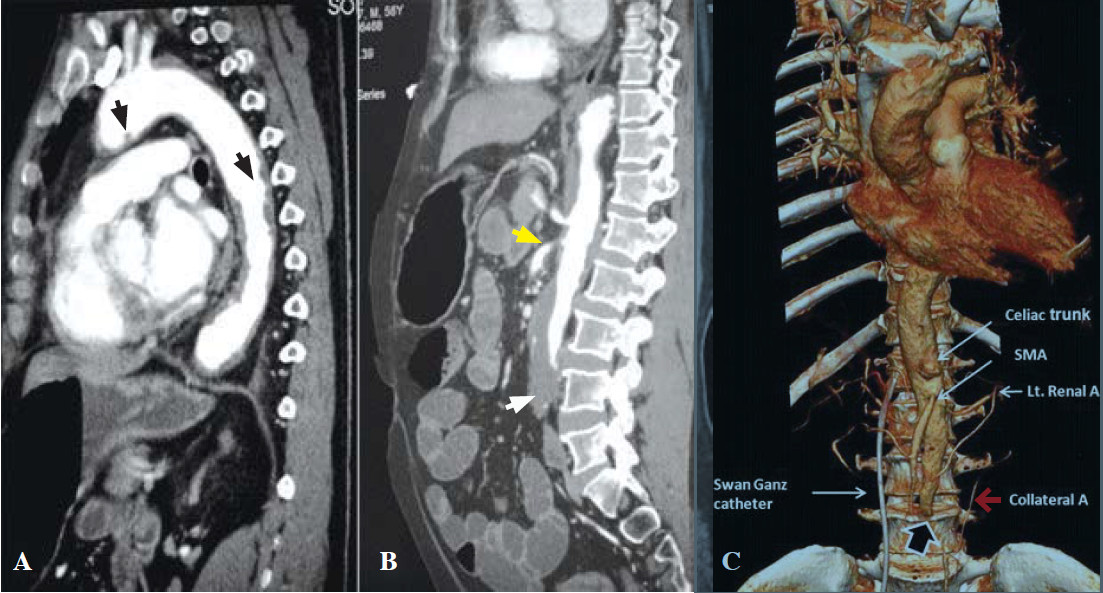
Figure 4:
The sagittal CT image shows multiple aortic ulcers (black arrow, A) extending from the arch along the descending aorta and mural thrombi occluded distal abdominal aorta (white arrow, B). The inferior mesentery is occluded. The celiac artery is patent; the superior mesenteric artery is marked as narrow at its origin (yellow arrow, B). The volume-rendered CT image (4C) shows an abdominal aortic occlusion (black arrow) with minimal collateral circulation from the retroperitoneal artery (red arrow, C).
Figure 5:
After 24 hours, the patient presented bluish feet caused by vascular occlusion.