Electronic ISSN 2287-0237
Formation of rice bodies in joints commonly occur in tuberculosis, rheumatic diseases and osteoarthritis. Sometimes rice bodies are found in synovial structures like tendon sheaths and periarticular bursa. Its occurrence always denotes the chronic state of the underlying disease. There are several hypotheses put forth to facilitate its etiology but there is no proof regarding its origin.1,2 Here we report a case where there was formation of rice bodies in the tenosynovium of extensor carpi ulnaris which healed completely after thorough surgical debridement.
A 45-year-old woman farmer presented to us with complaints of pain and swelling over the ulnar side of the extensor aspect of right wrist for 2 years (Figure 1-2). Swelling was initially small and later gradually progressed to attain the size at presentation. Earlier, the swelling was associated with mild pain only during work. Later as the swelling progressed there was an increase in pain and numbness over the ring and little finger. There were no complaints of polyar- thralgia or any symptoms of inflammatory back pain. The resultant restriction of activity caused the patient to seek treatment.
Clinical evaluation was suggestive of a lobulated swelling measuring about 4x2 cms which was cystic in consistency. Its margins were diffuse and extended proximally and distally. Fluctuation and translumination were positive which gave an exact picture of a dorsal ganglion except for its large size. Plain radiographs of the wrist merely showed a soft tissue swelling. Routine laboratory investigations and inflammatory markers such as erythrocyte sedimentation rate (ESR) and C - reactive protein (CRP) were within normal limits. Patient had a negative Mantoux test, rheumatoid arthritis (RA) factor and anti-cyclic citrullinated peptide (anti-CCP) immunoglobulin G (IgG).
Based on the findings, surgical excision was planned. A vertical incision over the entire length of the swelling was made. After superficial dissection, the lobulated ganglionic mass was found to arise from the tenosynovium of extensor carpi ulnaris. On opening the sac, numerous rice bodies were seen along with fibrinous material and straw colored fluid (Figure 3). Complete debridement of the inflamed tenosynovium was done with removal of all rice bodies (Figure 4). Specimen was sent for histopathology and culture.
Histopathology revealed presence of bulbous fronds of hyper- plastic synovial tissue with underlying intense chronic inflammatory cells like lymphocytes, plasma cells, multinucleated plasma cells and histiocytes in the fibrocollagenous stroma suggestive of chronic inflammation (Figure 5). Culture revealed no growth of any organism.

Figure 1: Dorsoulnar ganglion measuring 4x2 cms.

Figure 2: Lobulated swelling clearly seen from the lateral aspect.

Figure 3: Rice bodies seen along with fibrinous material and straw colored fluid.
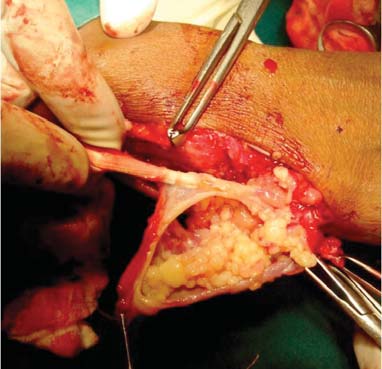
Figure 4: Extensor carpi ulnaris clearly seen during debridement.
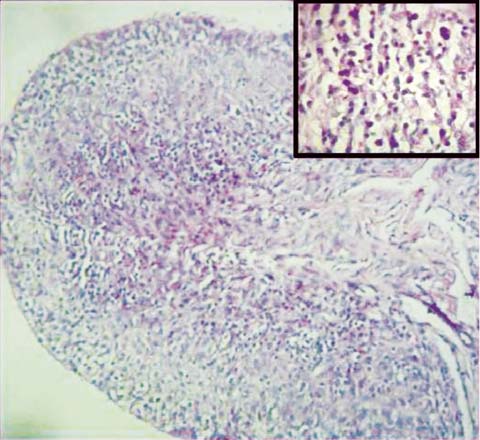
Figure 5: Histopathological slide showing hyperplastic synovial tissue with underlying intense chronic inflammatory cells (Magnified image shows multinucleated plasma cells).
The patient did not fit into the criteria for diagnosis of rheumatoid arthritis or peripheral spondyloarthropathies as it was an isolated issue of the extensor carpi ulnaris alone. Keeping the chronicity of this condition in mind an intensive therapy including anti-inflammatory drugs and disease-modifying antirheumatic drugs (DMARDs) were started. Six month follow up was uneventful with complete recovery of the condition.
Most authors attribute the formation of rice bodies to a chronic response to synovial inflammation.1-3 Literature states that rice bodies can occur either from the joints or any other synovial structures like periarticular bursa or tenosynovium.4,5 The condition is frequently associated with tuberculosis, rheumatoid arthritis, seronegative rheumatoid arthritis and sometimes osteoarthritis.6,7 Although extensor and flexor aspects of the wrist are the most common sites for tenosynovial inflammation, the site of occurrence varies. Reports reveal uncommon sites like biceps, semi- membranosus and tibialis anterior tendons.5,8 Rice bodies can also be associated with calcific material.9
In our case, tenosynovium of extensor carpi ulnaris was inflamed and gave a picture of an unusually large dorsal ganglion. Symptoms of numbness could be attributed to compression of the cutaneous branches of the ulnar nerve. Restriction of motion could be due to the unusually large size of the swelling. Thorough surgical debridement was the mainstay of treatment and care was taken not to leave behind any inflamed material.10 Similar to various reports in the literature, there was no recurrence following extensive surgical debridement.2-5,7,9,11
An unusually large ganglion is a response to tenosynovial inflammation but whether such persistent untreated conditions lead to rice body formation needs to be researched. Formation of villous folds, presence of focal lymphoid nodules, fibrinous exudates and plasma cell infiltration are all signs of chronic inflammation.11 The strong association between chronic synovial inflammation and formation of rice bodies cannot be ruled out. Its mere presence denotes the chronicity of the condition and the need for extensive debridement to prevent any recurrence. Such conditions are completely manageable and the patient can return to their best functional status.
Acknowledgements
We sincerely thank our Professor Dr C.S. Krishnamurthy for his guidance. We thank our Department of Pathology for providing us with evidence for our diagnosis.









