Electronic ISSN 2287-0237
The ruptured dissecting aneurysm of the renal artery is a rare condition. Previous articles demonstrate the rupture of an aneurysm by renal angiography as seen in 1990 by Cheng C et al.1 They found fibromuscular dysplasia of the media and subintimal regions at site of the aneurysm. Wilde V De. et al2 showed the site of the ruptured renal aneurysm into the renal pelvis by multidetector computed tomography (MDCT) after 2007, but the nature of the aneurysm was not described. We reported a case similar to Cheng C et al.1 described above but we demonstrated the aneurysm by computed tomography (CT). The patient underwent nephrectomy and recovered well. The pathological study of the aneurysm revealed a cystic medial degeneration and necrosis of the arterial wall.
A 58-year-old female with the chief complaint of acute colicky right flank pain not relieved by paracetamol came to hospital. Her past history was a colicky pain on the right side of the abdomen for the past year and a half, more painful when she was sleeping on her right side as she often did at night. She had asthma, relieved by a decongestant drug nasal spray. She had a history of hypertension with medication taken irregularly and she had no history of diabetes mellitus. No evidence of regular health checkups was noted. The physical examination on her admission showed the following: Temperature 37.3 °C; pulse 78 per min regular rhythm; BP 184/100 mmHg; oxygen saturation (O2 sat) 98%; good awareness; neither pale nor icteric. She complained of tenderness with questionable guarding at her right lower abdomen, and active bowel movement was noted. The femoral pulse was strong at both extremities, other organs were unremarkable, and the provisional diagnosis of acute appendicitis was given. A whole abdomen CT with contrast was preformed (Figure 1A - B), and after a complete CT examination, during her transfer to the ward, she developed severe right lower abdominal pain and abdominal distension. Her BP was 90/60 mmHg, one hour later, BP was undetectable, and heart rate was 80-100 per min, and O2 sat was 100%. There was no femoral pulse detected on either extremity but the carotid pulse was positive, she was alert, and underwent an abdominal exploration during full life support intravenous remedies. The operative findings were 500 ml hemoperitoneum and a large retroperitoneal hematoma on the right side extending to the left side and to the pelvic cavity.
Arterial blood was observed. After the blood clot was removed, a large ruptured extra-renal aneurysm was found, ligation and right nephrectomy were performed, and after the operation non oliguric renal failure occurred. The patient received the appropriate medical treatment and recovered four days post operation. She was discharged after 12 days post operation without any relapse. The histological detectable lesion of the aneurysmal wall is a cystic medial degeneration which is characterized by fragmentation and separation of elastic tissue and smooth muscle components of tunica media forming cystic spaces containing the amorphous extracellular matrix which is pale basophilia in hema-toxylin and eosin stained section (Figure 4), and pale blue in alcian blue stained section (Figure 5). Large scale loss of elastic (Figure 6) and muscular tissue (Figure 7) with blood-filed spaces (Figure 8) are present in some areas. There is no inflammatory infiltrate in these areas. Renal parenchyma shows segmental chronic pyelonephritis (Figure 9).

Figure 1A: CT image on arterial phase axial section reveals elongation of right renal artery encircled by a round homo- genous density which is representative of an aneurysm (see arrows) with compression of the renal pelvis and displacing laterally.
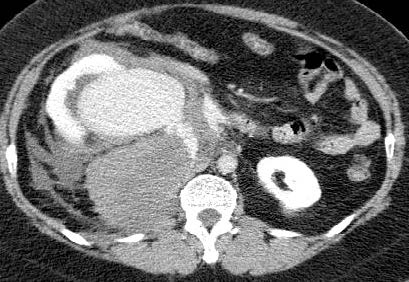
Figure 1B: CT image on delay phase axial section reveals contrast filled renal aneurysm perforating into perinephric region (see arrow).
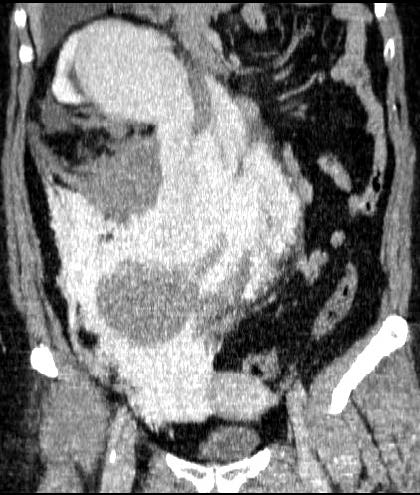
Figure 1C: CT image on coronal section on delay phase reveals the site of the renal aneurysm perforation into the perinephric space (see arrows).
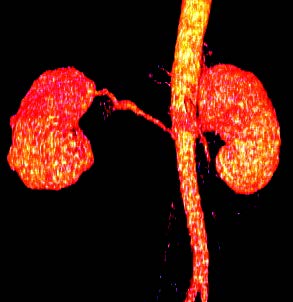
Figure 2A: 3D reconstruction of aorta and renal arteries reveal elongation and stretching of right renal artery.
The aneurysm and site of perforation are demonstrated.
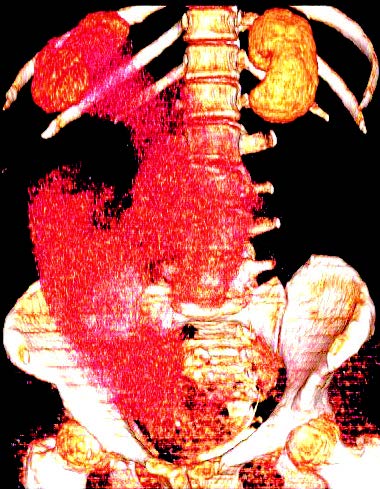
Figure 2B: 3D reconstruction demonstrates extensive hemorrhage from renal aneurysm into retroperitoneal
perinephric, right lumbar gutter and pelvic regions (see red color).
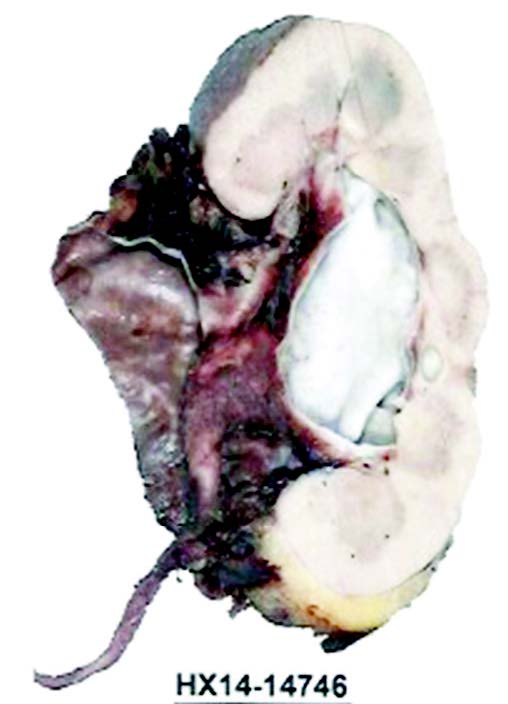
Figure 3A: Gross photograph of opened aneurysm of renal artery and dilated renal pelvis.
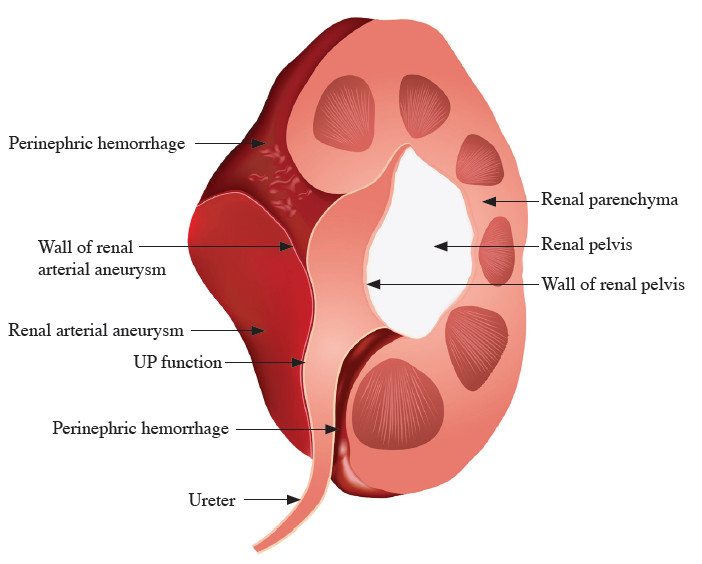
Figure 3B: Diagram corresponds to gross anatomy.
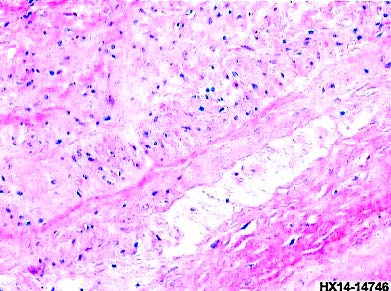
Figure 4: Cystic medial degeneration of wall of aneurysm, (hematoxylin and eosin x200) see arrows.
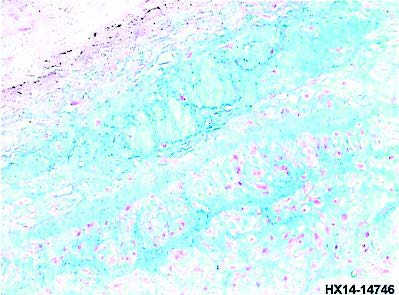
Figure 5: Cystic space containing extracellular matrix, (alcian blue x200) see arrows.
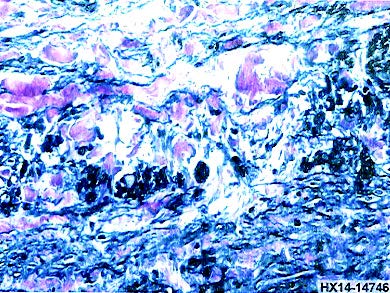
Figure 6: Fragmentation of elastic lamina, (elastic stain x200) see arrow.
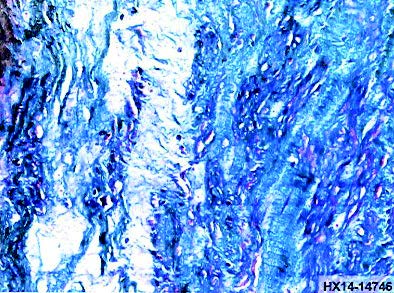
Figure 7: Fragmentation of smooth muscle component, (Masson trichrome x200) see arrows.
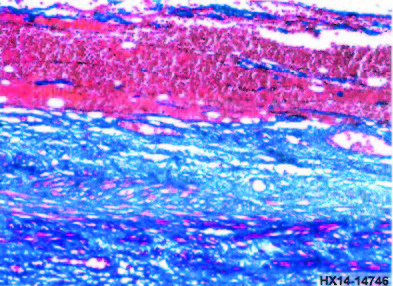
Figure 8: Blood-filled space in aneurysmal wall, (Masson trichrome x200) see arrows.
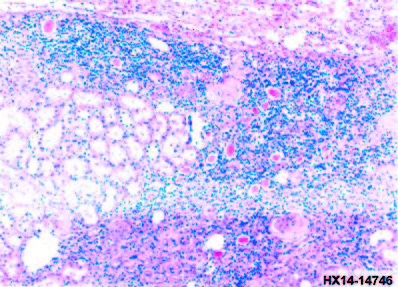
Figure 9: Segmental chronic pyelonephritis, (hematoxylin and eosin x100) see arrows.
Extra-renal aneurysms are relatively uncommon but may be observed more frequently now after the introduction of new non-invasive computed tomography examinations. These aneurysms divide into true and false aneurysms. A true aneurysm is due to atherosclerotic changes, fibro- muscular dysplasia or mesenchymal diseases. The false aneurysm is due to trauma, iatrogenic, Behcet’s disease and mycotic aneurysm. The etiology by histopathologic findings are:
The patient presented with a history of sudden colicky pain followed by rapid deterioration to a shock condition, the initial diagnosis is likely due to be associated with ruptured dissecting aneurysm of the aorta, renal artery or visceral artery. In this case, an urgent abdominal exploration was undertaken after a routine laboratory examination and contrast CT study were performed. The CT images (see Figure 1A - 1C and Figure 2A - 2B), show definite evidence of ruptured right renal aneurysm into the perinephric space, the renal pelvis is compressed by aneurysm and there is thin renal parenchyma and no arterial wall calcification. The gross appearance of the aneurysm is sacculo/fusiform type, when dissected perforates into the perinephric region. The gold standard investigation is selective renal arteriography however the processing for this examination takes longer and is a delicate procedure. CT examination of the abdominal aorta and its branch with contrast enhancement and 3D reconstruction is faster and is more precise in identifying the cause and location of the aneurysm. In this case, the point of perforation from an extra-renal aneurysm is demonstrated in serial CT images (Figure 1A - 1C and Figure 2A - 2B). The characteristic finding is sacculo/fusiform type and rupture into the perinephric region, the psoas muscle is compressed laterally and is not involved. The nature of this type of aneurysm may be due to either cystic medial degeneration or fibromuscular dysplasia. It is frequently found to be dissecting, and ruptured into the perinephric or renal pelvis.1,2 The histology may be due to fibromuscular dysplasia which is fibrous and muscular hyperplasia that infiltrates the tunica media resulting in vascular wall narrowing and weakening of the lumen. It could be cystic medial degeneration of the arterial wall which shows cystic degenerative changes with fragmentation of the smooth muscle and elastic lamina components. It is unlikely to be due to atherosclerotic changes because there is no evidence of calcified arterial wall, furthermore if renal aneurysm is the cause, aneurysms may occur also at other arterial sites, especially the internal carotid artery (prevalence of 8.5%).3 The predisposing causes are arteriosclerosis, congenital vascular malformation, harmatoma, pregnancy, trauma and underlying hyper- tension that has remained unresponsive to medical treatment.4 The clinical course is acute colicky flank pain and shock, microscopic red blood cells in urine may occur. The ruptured dissecting renal artery should be considered, emergency nephrectomy is unavoidable. The other possibilities are embolization of branch renal artery aneurysm (RAA), main renal artery with either ligation and bypass surgery or stent replacement.
Histological lesion of aneurismal wall of renal artery of this case is not fibromuscular dysplasia. The finding shows severe fragmentation of elastic and muscular components of tunica media with cystic medial degen- eration are similar to the dissecting aneurysm of aorta frequently accompanies Marfan syndrome. Lumsden el al4 reported 24 cases of renal artery aneurysm, of these most were caused by atherosclerosis (75% of cases), followed by fibromuscular disease (21% of cases) and Ehlers- Danlos syndrome (4% of cases).
A case report of a 58-year-old woman presenting with sudden right colicky flank pain and rapidly deteriorated to shock condition. CT images reveal sacculo/fusiform right renal artery aneurysm ruptured dissecting into the perinephric region. An emergency abdominal exploration, nephrectomy and evacuation of blood collection in perinephric region were performed, the patient recovered. The histology is due to cystic medial degenerative changes of the renal artery. The patient was given the recommen- dation to undergo a workup for other arterial aneurysms which may lead to perforation especially of the internal carotid arteries.









