Electronic ISSN 2287-0237
Hypertension is the most commonly found chronic illness that constitutes a major public health problem all over the world, causing people to meet untimely deaths. It has been estimated that by the year 2025 the number of adults who are stricken with hypertension will rise to 1.56 billion.1 Moreover, each year, the number of adults who died from hypertensive complications is almost eight million.2 Thus, hypertension is termed a “silent killer.” This is because during the initial stage of hypertension, there are no symptoms.3
Data from The Fifth Physical Examination of the Thai Population in 2014 has reported that the prevalence rate of hypertension is 24.7%, and it ranks fourth among the leading causes of death of the Thai population.4 The incidence rate of hypertension has increased to 66,567 persons per year5 and approximately one in five persons with hypertension have received treatment but cannot control their blood pressure levels (< 140/90 mmHg).6
At present, the health promotion of the world population emphasizes development of fundamental components of health literacy of individuals and practices that affect determinants of health. The World Health Organization has defined health literacy as various perceptive and social skills that determine individuals’ motivation and ability to access, understand, and utilize information to promote and maintain health.7-9 Health literacy is based on literacy which refers to the ability to read, write, speak, calculate, and solve problems to accomplish life goals and continue self-development.9,10 It has been documented 16% of the adult population in the world, or approximately 766 million people, lack basic literacy, and this affects their health literacy, leading to poor health.11,12
The concept of health literacy became clearer after Nutbeam (2008)13 has divided health literacy into three levels: functional health literacy, interactive health literacy, and critical health literacy. In Thailand, health literacy has been promoted as a national agenda in the 20-year national strategic plan, specified in the 12th National Economic and Social Development Plan (B.E. 2560-2564) with an aim to lead the population of the whole country to Thailand li style="text-align: justify;">The functional level of health literacy was subdivided into five aspects as follows:
Part 3: Scientific instruments.
The instruments used to evaluate clinical outcomes are weight scale, height scales and digital blood pressure machine.
Preparation stage
After the research proposal was approved by the Institutional Review Board on Research Involving Human Subjects of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, the researcher submitted a letter from the Graduate School of Mahidol University to Prachinburi Public Health Office and directors of the selected sub-district Health Promoting Hospitals (Wat Bot, Khok Mai Lai, Non Hom, Baan Toong Talumpuk, Mai Ked, and Nern Hom) to explain the research objectives and ask for permission and cooperation in data collection. The researcher studied the operations of the NCD clinic, including the number of patients with hypertension who sought treatment at the hospitals, and established rapport with the public health officers working at the selected sub-district Health Promoting Hospitals. In addition, the researcher trained the research assistants for one day on the instruments and data collection process. After that, the research assistants selected the subjects who met the inclusion criteria by randomly selecting from the database of patients with hypertension using a computer program until 368 subjects were recruited in accordance with the proportion of the patients with hypertension who sought treatment at each of the hospitals.
Implementation stage
The researcher met the subjects who were selected from the database of patients with hypertension, introduced herself, explained the research objectives and data collection procedures, conducted human subject protection, and asked for their cooperation in data collection. After the subjects agreed to take part in the study, the researcher asked them to sign the informed consent form. The subjects who were older than 60 years old had to be screened with the Short Portable Mental Status Questionnaire (SPMSQ) and they needed to have a score of at least 8 points to be eligible to participate in the study. Then, the researcher or research assistants assessed the subjects’ clinical outcomes including blood pressure levels, body weight, height, and waist circumference. The researcher also recorded the retrospective blood pressure levels of the subjects in the past three and six months from their medical records to calculate their mean blood pressure levels. After that, the subjects were asked to complete the questionnaires, lasting 30 to 45 minutes. As for the reading basic vocabulary questionnaire, there were 66 words for the subjects to read out loud. The subjects had to read the words one by one, spending four to five seconds on each word. If they were unable to read them or paused to spell them longer than the time specified, they would be asked to skip that word and considered they were unable to read them. In the end, the researcher checked all the questionnaires to ensure completeness, coded them, and thanked the subjects and gave them a token of appreciation.
Data analysis
It was discovered that there were only 360 questionnaires that were fully completed. A computer program was used in the data analysis. Descriptive statistics were employed to analyze data regarding demographic characteristics of the subjects in terms of percentage, frequency, mean, mode, minimum and maximum, and standard deviation. Furthermore, Chi-square test was utilized to analyze the relationship between selected factors and health literacy and clinical outcomes of the subjects
Part 1: Selected factors of the subjects
According to the study findings, more than two-thirds of the subjects, or 67.5%, were female. Half of them, or 50%, were older than 60 years of age, while 45% were between 40 and 60 years old, with the mean age of 59.29 years (SD = 10.89). The minimum age was 21, whereas the maximum age was 88 years old. All of the subjects were Buddhists, and 76.1% completed elementary education, followed by those who were uneducated and completed early secondary education, at 8.9% and 7.2%, respectively. In terms of occupation, more than one-third, or 36.7%, were agriculturists, 23.3% were wage earners, and 23.1% were unemployed or housewives. Nearly two-thirds of the subjects, or 65.6%, had their mean income lower than 5,000 baht per month. The minimum income was 1,000 baht, while the maximum income was 50,000 baht, with the mean income of 6,101 baht, and with 30.6% of the subjects having inadequate income. When considering their health status, it could be seen that 72.5% had co-morbidity, mostly hyperlipidemia, at 56.4%, followed by diabetes mellitus at 25.0%. Half of the subjects, or 50.3%, had been diagnosed with hypertension for one to five years, and 38.1% had been diagnosed with hypertension for six to ten years. In addition, 84 subjects, or 23.3%, had a role in their community, with 67.8% of them being a village volunteer and 21.1% being a village working committee member. Finally, with regards to the severity of hypertension as classified based on the seven-color ball guideline,30 almost three quarters of the subjects, or 73.6%, were in the dark green level (controlled hypertension), whereas 21.7% were in the yellow level (uncontrolled hypertension).
Part 2: Health literacy
It was found that the largest groups of subjects had functional and critical health literacy at an adequate level, making up 52.2% and 60%, respectively. To explain further, 66.4%, 85%, and 57.2% had scores demonstrating the need for assistance with health information, reading medical vocabulary, and seeking and accessing health information at a sufficient level. However, 53.1% and 60.3% did show inadequate level overall health literacy and interactive health literacy.
Part 3: Clinical outcomes of persons with hypertension
The study findings showed that the mean systolic blood pressure level was 131.83 ± 12.30 mmHg. Moreover, more than one-fourth of the subjects, or 26.4%, were unable to control their systolic blood pressure (with their systolic blood pressure exceeded 140 mmHg.). Their mean diastolic blood pressure level was 78.66 ± 7.83, and 8.6% of the subjects were unable to control their diastolic blood pressure (with their diastolic blood pressure exceeded 90 mmHg.). The subjects’ mean body mass index was 25.27 ± 4.13 kg/m2, and 41.1% of them had body mass index at the obese level (25- 29.9 kg/m2 and 10.8% of the subjects had body mass index at the very obese level (>30 kg/m2). Finally, almost two-thirds of the subjects, or 63%, had waist circumference longer than the standard criteria (longer than 80 centimeters in females and longer than 90 centimeters in males), making up 78.4% and 21.6% of female and male subjects, respectively.
Part 4: Hypothesis testing
Table 1: Relationship between selected factors and health literacy of the study sample (n = 360)
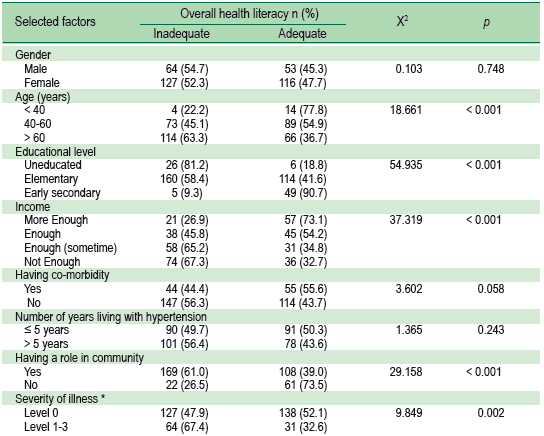
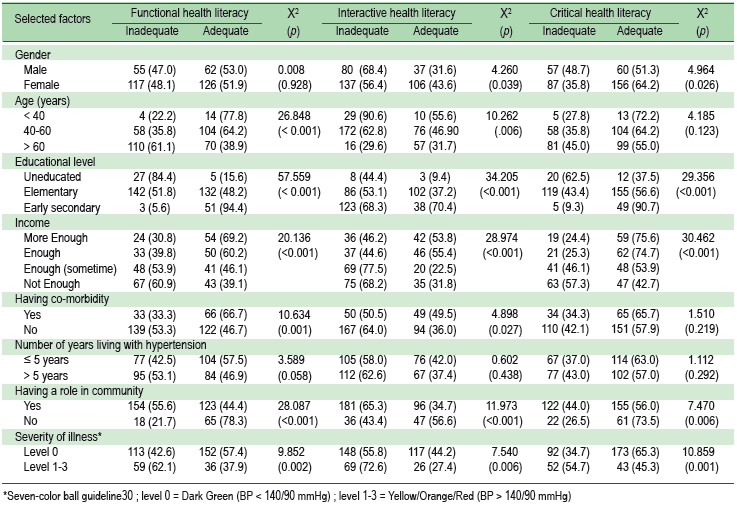
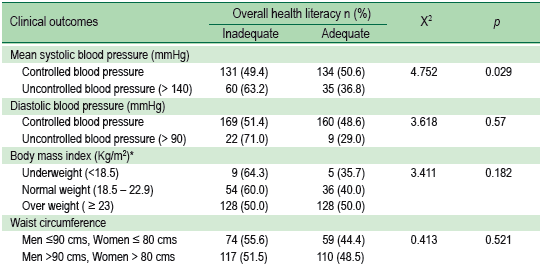
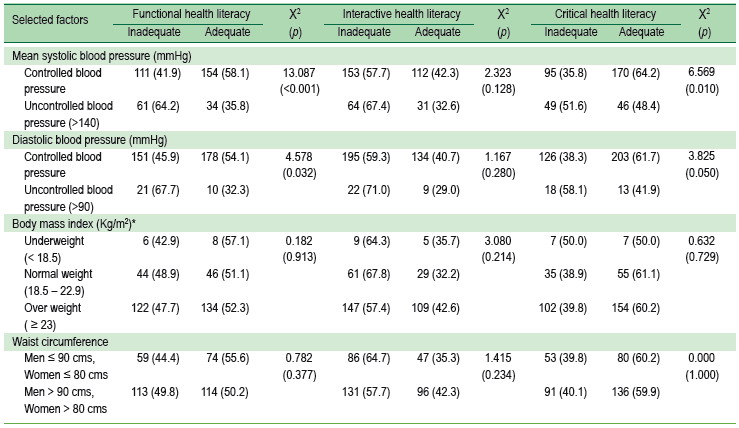
Table 2: relationship between health literacy and clinical outcomes of the study sample (n = 360)
According to the study findings, more than half of the subjects or 53.1%, had an inadequate level of overall health literacy. This was consistent with the finding of a previous study that health literacy of the people to adhere to the ABCDE principle was not good enough31 and that an individual who has insufficient or a low level of health literacy has restrictions in basic factors for learning, lacking awareness, and overlooking learning about self-care.32
When analyzing different levels of health literacy, it could be seen that 52.2% of the subjects had adequate health literacy. It has been found that most of the subjects had functional health literacy in the following five aspects—need for assistance with health information, reading basic medical vocabulary, and seeking and accessing health information, at 66.4%, 85%, and 57.2%, respectively. As for reading and understanding numbers and understanding hypertension, the subjects’ health literacy was not sufficient, at 91.7% and 93.6%, respectively. Results from our study showed that the prevalence was particularly high amongst subjects: 1) who only completed education of elementary school and below; 2) whose income lower than 5,000 baht per month and below; 3) who have inadequate income; 4) aged 60 years and above; and 5) who do not have any role in their community. In addition, 48.9% of the subjects aged 60 years or older had only completed education of elementary school or below. This may explain the prevalence of low health literacy as it may be due to these factors. The findings were consistent with several surveys of adult health literacy, which reported that the most common socio-demographic features associated with health literacy were education level, age, income, and having a role in the community.16,21,22,25
The findings of the present study supported the research hypothesis as it was found that selected factors of educational background, income, community roles, and severity of illness were related to health literacy (functional, interactive, and critical health literacy) with statistical significance (p < 0.01). Previous studies have also reported that education was related to health. This could be explained by the fact that individuals who have sufficient health literacy or who are educated highly enough can have more perception of hypertension.11 The Institute of Medicine has pointed out that health literacy depends on an individuals’ encounter with health situations including healthcare systems, educational systems, social factors, and cultures at home, in the workplace, and in the community.12 Health literacy enables people to better understand healthcare and adopt correct practices. In this study, 73.6% of subjects with hypertension were at the dark green level of the seven-color ball guideline30 that is, their blood pressure level was 140/90 mmHg., and they had to take medication to control their blood pressure level, which was the lowest level of severity.33 As for this group of subjects, 52.1% had a sufficient level of overall health literacy, whereas 32.6% of the subjects were at the yellow/orange/black level. Such findings yielded support to the findings of Thanasugarn C and Neelapaichit N33 that more patients at Level 0 (dark green) had a sufficient level of health literacy compared to those at levels 1-3 (yellow/orange/red). Thus, the seven-color ball guideline30 should be used to monitor, control, and prevent hypertension through health behavioral modification and the ABCDE principle.34
The findings of the present study support the research hypothesis that clinical outcomes of mean systolic blood pressure and diastolic blood pressure were related to health literacy with statistical significance (p < 0.001 and p < 0.05, respectively). Blood pressure examinations are generally conducted to make people know their own blood pressure levels so as to appropriately control them.35 In other words, when people have knowledge about the appropriate levels of blood pressure, they are able to make correct decisions and carry out self-management to control their own blood pressure levels.36-38
In summary, the study findings showed that health literacy referred to levels of knowledge and the ability of the individual to screen information to make a decision about self-care practices. In order for community nurse practitioners to access the people, they need to understand their nature, ways of life, and their environment and how much they facilitate health promoting activities to ensure continuity and sustainability. Health literacy can be utilized to ensure that people can appropriately access, understand, and use the information with suitability to their contexts. A key factor that contributes to the success of the health system is healthcare personnel’s health literacy including policies related to health literacy, use of instruments to assess health literacy, and application of technology and innovations to ensure that Thai society is a society of health literacy.
This study suggested that healthcare teams should provide health information and hypertension education programs with a focus on target populations, particularly to persons with inadequate health literacy including the elderly, those with low education and of low income. They should communicate effectively and make health information accessible and in a language that is easy-to-understand in order to promote proper decision-making and lead to good clinical outcomes. Further research needs to focus on the developed program for enhancing health literacy especially for low health literacy people such as using oral and visual communication to convey necessary medical information through photo novella, one-onone teaching, audiotapes, videotapes or computer multimedia.
I would like to thank 6 sub-district Health Promoting Hospitals (Wat Bot, Khok Mai Lai, Non Hom, Baan Toong Talumpuk, Mai Ked, Nern Hom ) in Muang District, Prachinburi Province, for their help and contributions to this research.









