Electronic ISSN 2287-0237
The causes of the noise-induced hearing loss are either from exposure to loud noise (continuous noise or intermittent noise) for long periods of time when the level of loudness is greater than or equal to 85 dBA (8-hour time- weighted average)1 during working hours or from exposure to short bursts of impulse noise levels (over very short period of time). That is to say, exposure to continuous noise or intermittent noise for a long time can cause hearing loss; the most affected frequency is 4000 Hz, with the precise pattern depending on the spectral characteristic of the exposure,2 gradually increasing over time (after 10-15 years). After this time, if there is still noise exposure,hearing loss slows down due to the higher hearing threshold.3 An exposure to impulse noise can result in ear pain, eardrum perforation and sudden hearing loss. The position of the noise notch depends on the location of the hair cells in the cochlea destroyed by the frequency, and the size of the ear canal. In early noise-induced hearing loss, the average hearing thresholds at the lower frequency (500, 1000, 2000 Hz) is better than the average threshold at 3000, 4000, 6000 Hz and at the 8000 Hz is better than the lowest point of the notch which is different from the presbycusis, which is found to have high frequency hearing loss with a down sloping pattern without recovery at 8000 Hz.1 In the elderly, hearing loss is also caused by age (presbycusis), and it is often necessary to compare current readings with earlier audiograms performed previously, as the bulging curve should be considered according to the age range.1,4
WHO has determined that employees working in the industry must not experience exposure to loud noise at levels no higher than 85 dB for not longer than 8 hour a day, five days a week1,5 in order to prevent hearing loss. Noise-induced hearing loss effects are seen mainly at 3 kHz, 4 kHz and 6 kHz with a significant noise notch while at 8 kHz, the higher threshold, hearing is more preserved.1 However,factors to consider include age, gender, sensitivity of the hair cells responding to loud noise and time of noise exposure both during work1 and outside of work.
This study is a cross sectional study aiming to study the prevalence of noise-induced hearing loss in 50 ambulance nurses working in ambulances of the Bangkok Hospital headquarters from October to November 2015.
The inclusion criteria were as follows:
1. Both male and female nurses exposed to loud noise in the ambulance, going with the ambulance.
2. Aged 20-60 years old.
3.. Willing to participate in the study.
There were exclusion criteria as follows:
1. Having respiratory illness on the day of the audio- metric examination.
2. Having impact cerumen which cannot be removed on the day of the hearing test.
3. Not cooperating in the audiometric examination.
The samples signed a consent before the study was started.
Method of Study
A nurse must not have been exposed to loud noise before the audiometric examination for at least 12 hours prior to examination.6
1. The participants were required to answer the ques- tionnaire including provding data on age, gender, duration of noise exposure each day, the knowledge about the dangers of noise and the use of hearing protective devices.
2. The doctor who conducted the research performed the otoscopic study, checked the ear canals and eardrums.
3. The audiogram was done at the frequencies of 250, 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz using screening audiometer, Micromate 304, Interacoustic AC40 and Amplaid A321 brands, which had been calibrated in the sound proof booth before the audiometric examination.
4. The noise in the ambulance was measured during the trip using a sound level meter (DAIICHI and 3MTM Sound Detector SD-20) attached to the seats of the nurses in the ambulance.
5. Noise exposure was also measured throughout the trip with the ambulances using a noise dosimeter (QUEST-200) attached to the nurse’s belt and the microphone was attached to the collar close to the ears.
Data collection
1. An audiogram was done to investigate the noise notch. The criteria for diagnosis of noise-induced hearing loss:
a) A history of long or sudden noise exposure mentioned above.
b) According to physical examination, normal eardrums and ear canal.
c) All audiogram are collected and if noise notch2 was found at 3000 Hz, or4000 Hz, or 6000 Hz which is greater than or equal to 20 dB and greater than 2000 Hz and 8000 Hz considered positive finding (see Figure 1).
2. The noise in the cabin of the ambulance was measured by using a sound level meter.
3. The noise exposure was measured by the noise dosimeter and was measured by the noise dose (%) throughout the trip.
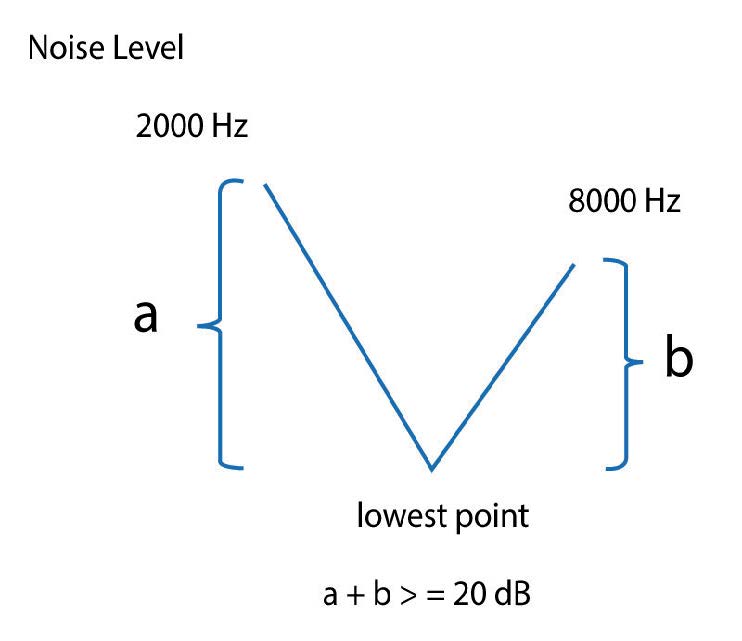
Figure 1
Data analysis
1.The prevalence of noise-induced hearing loss was calculated from the percentage of nurses participating in the noise notch study.
2.The descriptive statistics were used to analyze the characteristics of the samples, including the percent- age of gender, the average age,the average duration of noise exposure at work and the use of hearing protective devices in the emergency department at Bangkok Hospital headquarters.
A screening audiometric test was conducted with 50 nurses who had met the inclusion criteria as mentioned above. There were 18 (36%) male nurses and 32 (64%) female nurses. The average working duration was 2.6 years and the average age was 31 years old (Table 1). Underlying diseases: 2 cases: allergy, 2 cases: high blood pressure, ear diseases: 2 cases: otitis externa.
There were 30 staff already exposed to loud noise at work as they had been working also with ambulances of the other hospital institutions (BDMS group:Bangkok Hospital, Samitivej Hospital, Phyathai Hospital etc.). It was also found that 44 (88%) of the nurses did not use hearing protective devices (Table 2). It was found that 46 (92%) of the nurses had normal hearing while 4 (8%) of the nurses had hearing problems (see Table 3). From the 4 nurses with an abnormal audiogram, the noise notch was found in three of them while it was not found in one of them (Table 4). More than 80% of the nurses knew that loud noises greater than 85 dBA can damage hearing (the average of noise in the ambulance of the hospitals in BDMS group was less than or equal to 85 dB) see Figure 2. Most of the staff were exposed to loud noise for less than two hours each day according to the rotation of the schedule (Figure 3).
Table 1: Demographic characteristics of the study of hearing loss in ambulance nurses (n = 50).
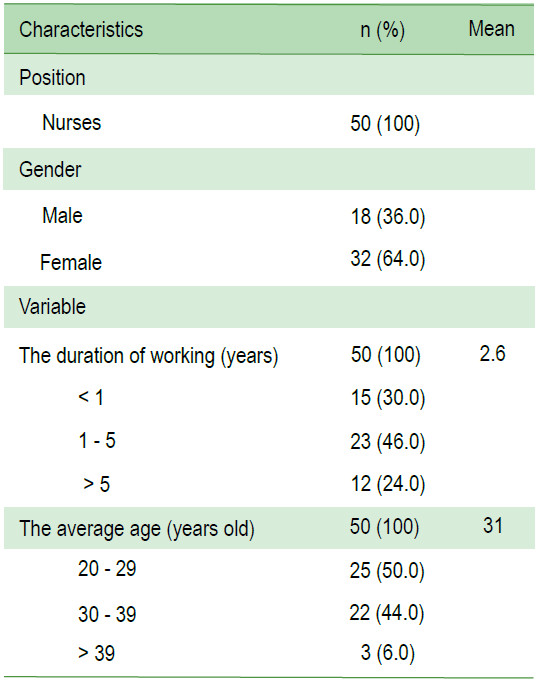
Table 2: Past history of noise exposure, ear problems and use of hearing protective devices (n = 50).
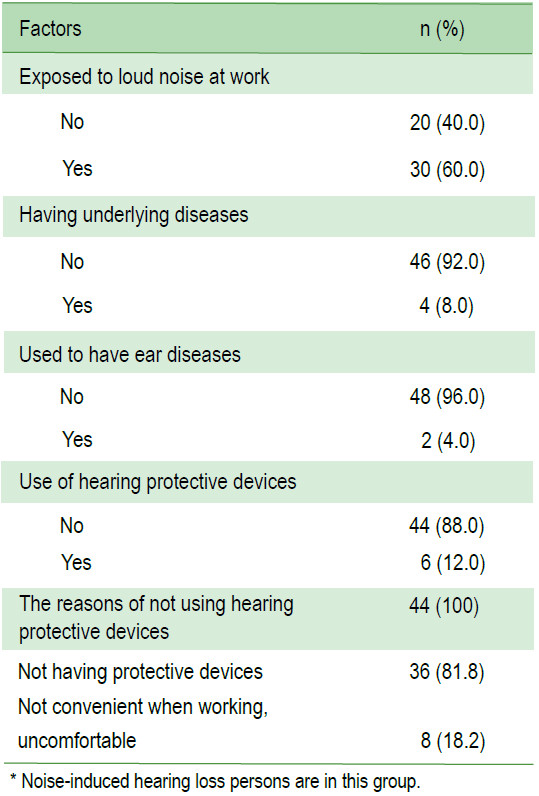
Table 3: Result of screening audiometric test in sound proof booth (n = 50).
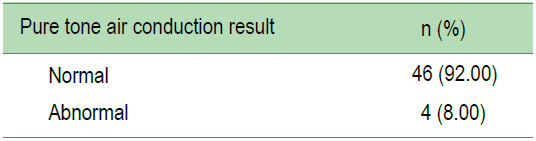
Table 4: Numbers of Noise notch in any frequency (n = 4).
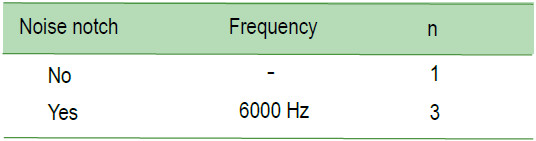
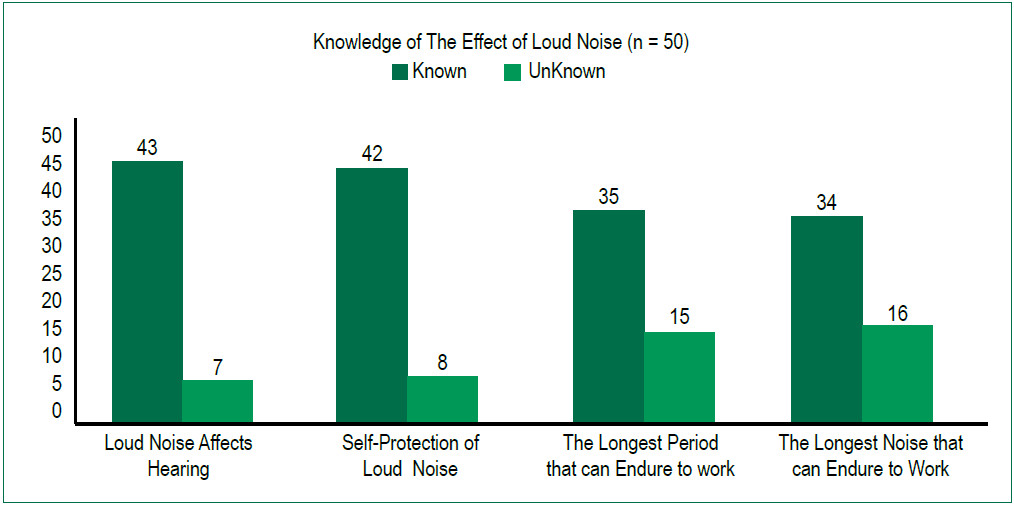
Figure 2: Knowledge of the effect of loud noise.
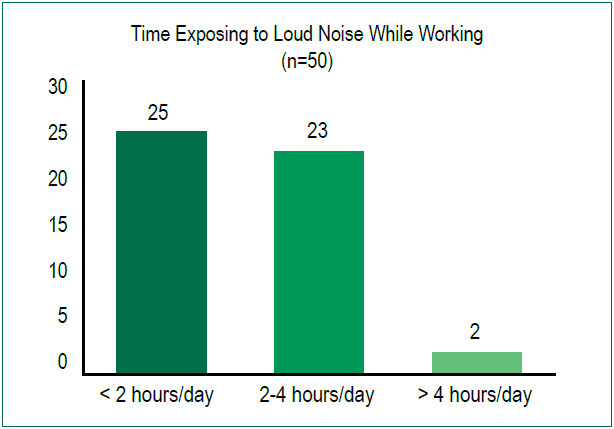
Figure 3: Assessment of working environment.
The average noise level in the cabin of the ambulance in the Bangkok round trips was 78 dB. The ambulance nurses were mostly exposed to loud noise for around 1-2 hours and the noise level in the cabin of the ambulance was less than or equal to 85 dB (the LMAX* =119 dB for a very short time (a few seconds). The individual noise exposure was measured throughout the trip by each ambulance nurse with the noise dosimeter, and it was recorded when the noise was greater than 80 dB. The ambulance nurses in the Bangkok round trip were exposed to an average noise dose = 1.3% (see 4A). Six out of the 20 ambulance nurses were exposed to noise higher than 85 dB (see 4B).
The average noise in the cabin of the ambulance from Bangkok to other provinces and returning to Bangkok was 82 dB. The ambulance nurses were mostly exposed to loud noise for around 1-5 hours and the noise level in the cabin of the ambulance was less than or equal to 85 dB, with the LMAX* =140 dB for a very short time (a few seconds). The individual noise exposure was measured throughout the trip by each ambulance nurse with the noise dosimeter, and it was recorded when the noise was greater than 80 dB. The ambulance nurses from Bangkok to other provinces and returning to Bangkok were exposed to an average noise dose = 3.4 % (see 5A). Nine out of the 20 ambulance nurses were exposed to loud noise of more than 85 dB (see 5B).
*LMAX is the maximum noise level measure over a time period
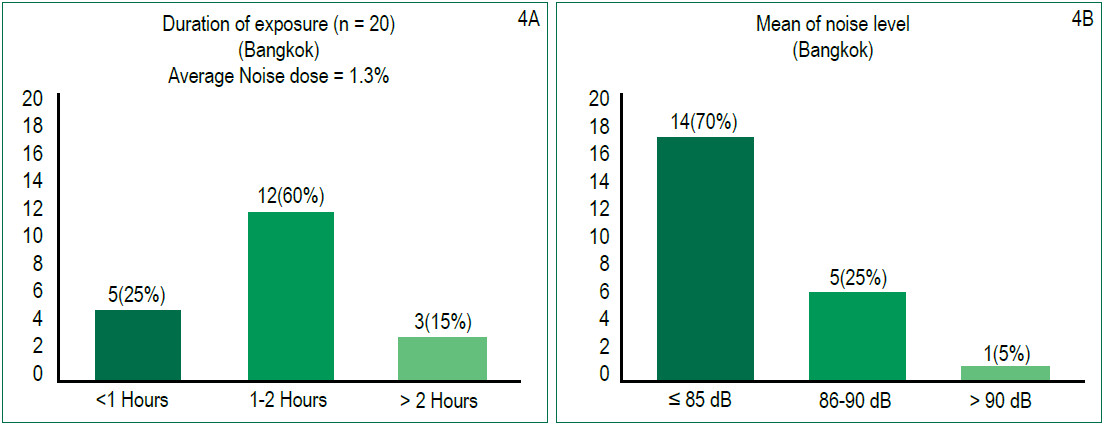
Figure 4: Nurses’ exposure to loud noise in ambulances over 20 round trips in Bangkok.
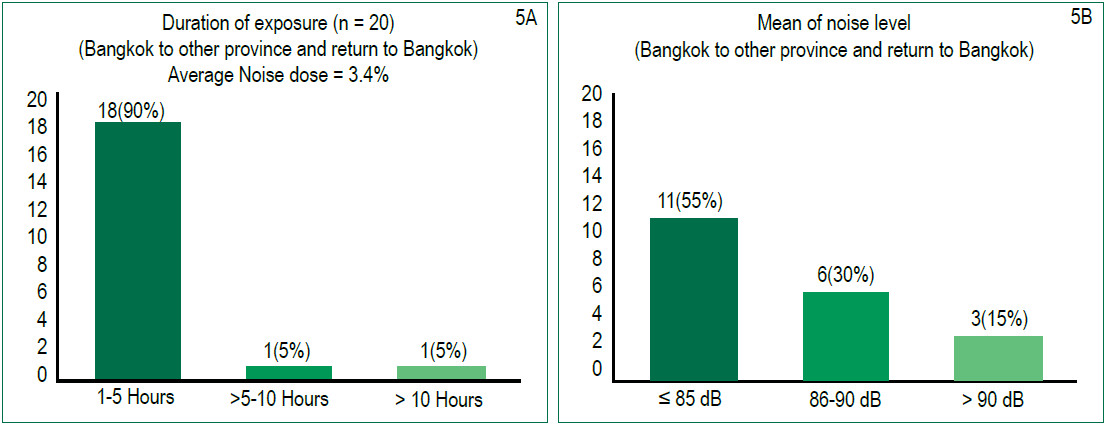
Figure 5: Nurses’ exposure to loud noise in the ambulances over 20 round- trips from Bangkok to other provinces and returning to Bangkok.
The results of the study revealed that there was evidence of noise-induced hearing loss of the ambulance nurses working in the ambulance with the loud noise greater than or equal to 85 dB. Although some nurses working at the emergency room and going with the ambulance have been working at Bangkok Hospital headquarter for a short period, som e had also previously worked at the emergency department s of other hospitals for several years. Therefore, it can be concluded that the cause of noise-induced hearing loss presented in Table 1 was indeed noise exposure. So, any hearing conservation program1,6 is useful to prevent new cases of noise induced hearing loss in other nurses and to prevent further worsening of hearing loss for those who are already experiencing hearing impairment. However, during the traffic congestion, when it is often necessary to use a siren, the noise in the cabin of the ambulance is greater than 100 dB and sometimes reaches 119, 140 dB in a very short period of time. That is to say when the ambulance moves very slowly and when the siren is used, the noise bursts reach higher levels than normal. As ambulances traveling from Bangkok to other provinces and returning to Bangkok face traffic jams very frequently, so the ambulance nurses in these services are exposed to loud noise at higher rates than nurses providing services within Bangkok round-trips (Figure 4,5).
Suggestions for reducing loud noise exposure
1. Solving the source of the noise:
a) Changing the location of the siren to the front of the ambulance, sitting away from the siren as far as possible and controlling the noise by adjus ting to the proper noise level.
b) Adequate insulation to the walls of the cabin.
2. Planning the schedule of the ambulance nurses properly to prevent exposure.6
3. Using hearing protective devices, designed to hear normal speech with a microphone attachment.
Note: that Thai regulation law6 requires staff to have an annual audiogram check.
The prevalence of noise-induced hearing loss of ambulance nurses was 6% according to our study. It is recommended as a precaution that all ambulance nurses need to participate in hearing conservation programs.
I would like to thank all staff and volunteers for their help and contributions in making this research a success. This study was funded by the Bangkok Health Research Center, Bangkok Hospital.









