Electronic ISSN 2287-0237
Giant cell tumor of tendon sheath (GCTTS) or localized tenosynovialgiant cell tumor is the most common lesion of giant celltumors.1 GCTTS usually involves upper limb especially small jointsof the fingers and less commonly occurring in wrist and lower extremities.Most patients frequently present with a gradually growing painless masswith normal adjacent skin. On histologic examination, tumor is composedof various populations of cells, including mononuclear stromal cells,osteoclast-like multinucleated giant cells, lipid or hemosiderin-laden foamycells. Although GCTTS is a common soft tissue tumor with distincthistologic features, it can be disregarded and misdiagnosed as other mimiclesions especially when originating in uncommon locations. Like this casereported, we present a case of GCTTS in the unusual site of leftsupraclavicular region, which is clinically suspected to be a pathologic lymphnode. To our best knowledge, there is no previous case report of GCTTS inthis location in literature.
We report a case of 26-year-old male patient, who presented withasymptomatic left supraclavicular mass for a year. Clinical findings weresuspicion of pathologic lymph node. Then, fine needle aspiration forcytology was performed and revealed dispersed single histiocyte-like cells,exhibiting round to oval, eccentrically located nuclei, evenly distributednuclear chromatin, inconspicuous nucleoli, and scant granular cytoplasm.Osteoclast-type multinucleated giant cells and hemosiderin-ladenmacrophages were also found in minor population, but neither polymorphouspopulation of lymphoid cells nor the background of necrosis wasdemonstrated. No atypical cellular change or abnormal mitotic figure wasdisplayed (Figure 1). These cytological findings were inconclusive and thepossibility of granulomatous inflammation could not be entirely excluded.However, physical examination and chest radiography did not show anysupporting evidence of tuberculosis. At a later time, surgeon excised thisnodule for histologic examination. Microscopic findings demonstratedwell-demarcated oval mass with fibrous septa. The tumor cells were apolymorphous population, comprising of osteoclast-like multinucleated giant cells, mononuclear stromal cells, hemosiderin-ladenmacrophages and some xanthoma cells without cytologicalatypia, lymphoid cell proliferation or tissue necrosis. Mitoticnumber was 0-1 per 10 high-power fields (HPF). Theseosteoclast-like multinucleated giant cells and xanthoma cellsare positive for CD68 by immunohistochemistry (Figure 2).The pathologic diagnosis was giant cell tumor of tendon sheathat left supraclavicular region. Patient had good post-operativesymptoms. During five-year follow-up, no local recurrencedeveloped.
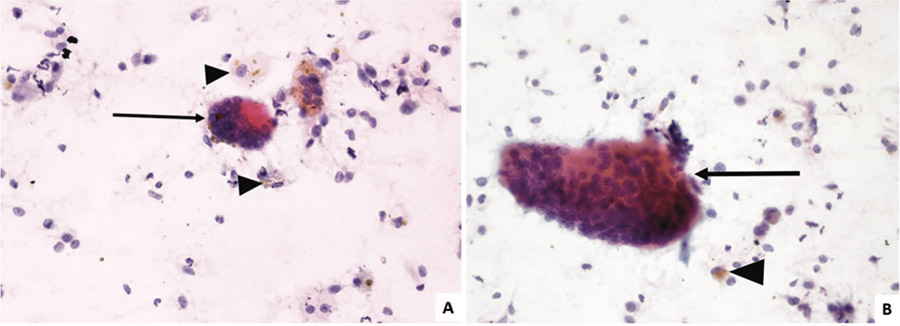 Figure 1: Cytological findings of GCTTS with dispersed histiocyte-like cells, multinucleated giant cells (arrow) andhemosiderin-laden cells (arrowhead) (A-B: Papanicolaou stain, x400)
Figure 1: Cytological findings of GCTTS with dispersed histiocyte-like cells, multinucleated giant cells (arrow) andhemosiderin-laden cells (arrowhead) (A-B: Papanicolaou stain, x400)
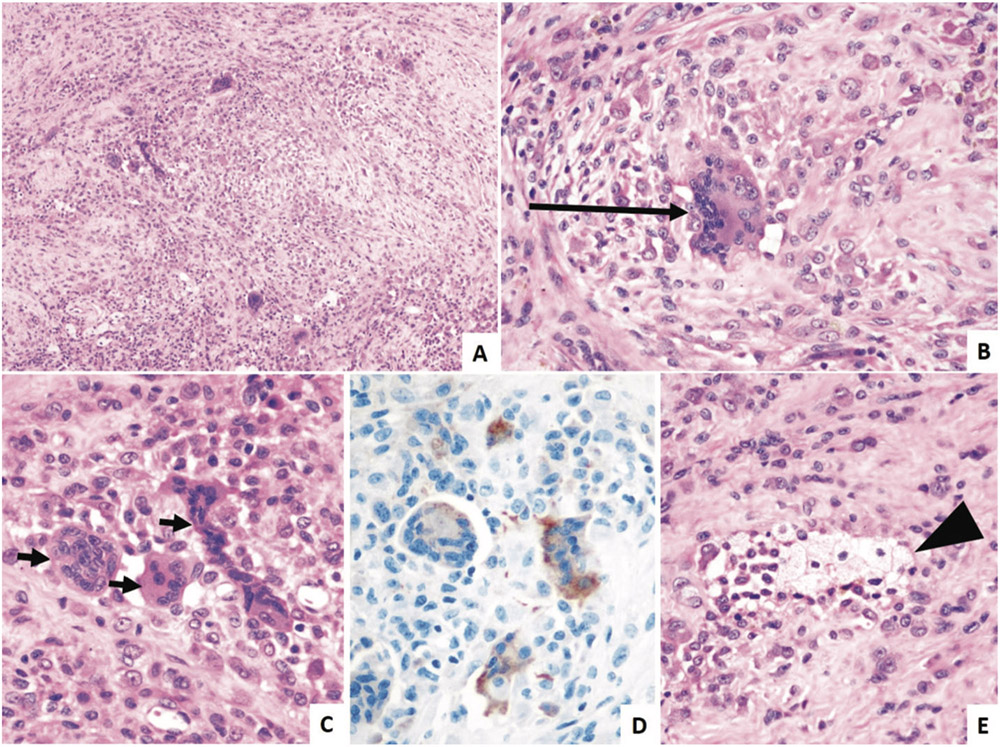
Figure 2:Microscopic findings of GCTTS (A-C) various population of cells in tumor, composing of scattered mononuclearstromal cells and osteoclast-like multinucleated giant cells (arrow) (A: hematoxylin-eosin stain, x100; B-C: hematoxylin-eosinstain, x400); (D) Osteoclast-like multinucleated giant cells are positive for CD68 (x400); (E) aggregates of xanthoma cells(arrowheads) in tumor (hematoxylin-eosin stain, x400).
Giant cell tumor of the tendon sheath have been recentlyknown as localized type tenosynovial giant cell tumor, andmost commonly occurred in the small joints of hands andfeet.1-2 Some studies also reported GCTTS at knee,periungual, palmar and shoulder regions.3-6 Cytologicalfeatures are unique and are composed of two main components,including stromal cells and multinucleated giant cells.2,7 Firstare the stromal cells or histiocyte-like cells that appear roundto fusiform, eccentrically placed nuclei, even chromatindistribution, single micronucleoli and a small to moderateamount of cytoplasm with dispersed individual cells orloosely aggregated sheets.2,7-9 Binucleation, nuclear groove orintranuclear pseudoinclusion may be illustrated in somecases.2,8,10 Multinucleated giant cells are another main featureof GCTTS. They usually contain 3 to more than 50 nuclei ineach cell with amphophilic cytoplasm.2,7,9 Other features,advocating GCTTS diagnosis, are hemosiderin-ladenmacrophages, xanthoma cells and myxoid background.2,7,9,11According to these features in those prior studies, almost allfindings could be found in our presented case, comprisingstromal cells, multinucleated giant cells and hemosiderin-ladenmacrophages. Nevertheless, xanthoma cells and myxoidstroma were not prominent.According to the histopathology, differential diagnosis ofGCTTS includes inflammatory process, particularlygranulomatous inflammation, or neoplasm (such as pigmentedvillonodular synovitis (PVNS), giant cell tumor (GCT) of softtissue or metastatic carcinoma).7 Especially unique anduncommon location, granuloma or metastatic giant cell richcarcinoma should also be highly considered and distinguishedfrom GCTTS. PVNS is usually found in large joint space withill-defined infiltrative margin. GCT of soft tissue has moreuniform distributed giant cells through the lesion. From theseformer statements, PVNS and GCT of soft tissue are lesslikely in our case. As could be seen in the reported case,numerous histiocyte-like cells with focal aggregatesand frequent multinucleated giant cells may resemblelymphohistiocytic aggregates in granuloma, having moreincidence than GCTTS in supraclavicular region. However,scant lymphoid cells and no necrotic background wereunlikely to support the diagnosis of granulomatous inflammation.Therefore, cytological diagnosis should be careful in giant cellrich lesion with strict diagnostic criteria to prevent the misleadingdiagnosis for unnecessary treatment.
Although GCTTS have specific morphologic features todiagnose them, it may not be recognized, however, when itoccurs in an unusual region and may probably mislead toother mimickers. Based on our knowledge, there is no priorreport of GCTTS in this area and few studies of thesetumoral cytological features. This reported case demonstratesanother GCTTS in supraclavicular area, suggesting concernof the cytological diagnosis of its mimics in uncommonlocation.









