Electronic ISSN 2287-0237
Diabetes is a major health problem worldwide, including in Thailand.1The prevalence rate has been increasingly rising from 8.3% in 2017and is expected to reach 10.8 % in 2045. Similarly, approximately 4.2 million Thai people were diagnosed with type 2 diabetes (T2DM) in2017.1,2 About 79% of all people with diabetes are unable to control bloodsugar leading to many complications including cardiovascular diseases,neuropathy, retinopathy, and nephropathy resulting in poor quality of life,high healthcare expenses, and approximately 30,000 people deaths annually.2-4 Therefore, explicit managements of diabetes is needed.
To achieve glycemic control targets, people with diabetes should betaking medication and modifying lifestyle activities, especially controllingdiet and ensuring adequate exercise.3 However, these may be difficult tocontinuously perform since a study reported that Thai people with diabetesconsumed an amount of carbohydrate per day that is more than the recommendedamount causing obesity and hyperglycemia.4 Moreover, lack of exercise cansignificantly accumulates abdominal fat and this is a predominant cause fordeveloping insulin resistance leading to T2DM and its complications suchas cardiovascular diseases.5,6 Thus, people should be encouraged to exercisemore in order to burn calorie intake as this is beneficial for improvingglycemic control.7 However, approximately 42% rural Thai people did notperform exercise and do have an inactive lifestyle8 because of lack of timeand poor exercise infrastructure.9 Thus, a strategy promoting continuouslyexercise should be developed in a convenient and practicable approach.
Currently, an arm swing exercise (ASE) is recommended as a governmentpolicy and is a well-known and practical method to promote physicalactivity.10 Performing ASE can encourage body movement integrated withmeditation, and this has benefits for glucose expenditure in muscle and i ncreased insulin sensitivity.10,11 The traditional arm swingexercise (TASE) has shown several advantages in numerousprevious studies including reduced HbA1c level, waistcircumference (WC), body mass index (BMI), and stress.12-15However, the TASE focuses on the upper part of the body. Itshould be more beneficial if researchers modify TASE to amodified arm swing exercise (MASE) using the lower part of thebody simultaneously and it has been claimed that this stimulateslymph nodes leading to an increase in cytokine affecting insulinactivity. This may assist in enhancing the level of glucose uptakein muscle to achieve glycemic control.16
Thus, MASE should be applied to promote hip and kneejoint movement and muscle contraction including abdominal and quadriceps. However, a limited study revealed that MASEperformed for 30 mins, 6 day/week for 12-week was able toreduce WC, but this exercise pattern could not improve fatmass and BMI in people with metabolic syndrome.16 TheMASE program should be further studied integratingBandura’s concept through four resources including: masteryexperience, vicarious experience, verbal persuasion andphysiological and effective states17 in order to enhancecontinuously performing exercise in people with T2DM asshown in Figure 1. Therefore, this present study investigatedthe effects of the MASE program on CPG, BMI, visceral fat,and skeletal muscle in people with uncontrolled T2DM. Thefindings could assist to control blood sugar and prevent diabeticcomplications.
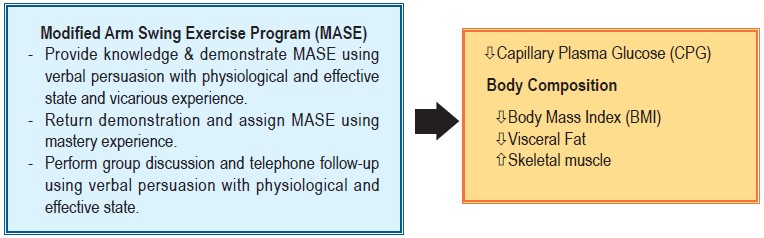
Figure 1: Conceptual framework of the MASE study
A quasi-experimental research: one-group pretest-posttestdesign conducted people with T2DM at the Ban Phai RongWua Sub-district Health Promoting Hospital, Suphanburiprovince, Thailand during December of 2016 to April of 2017.
Potential participants meeting the inclusion criteria:
The exclusion criteria consisted of performed MASE < 90minutes (mins)/week, missed appointments, referred tohospital or adjusted medication.The sample size was determined based on Power Analysisusing G*Power software sufficient for Repeated MeasureANOVA statistics with statistical power at 0.80, p at 0.05,effect size at 0.33 according to a previous study18 obtaining 23participants. Attrition rate 25% was added, so 30 people withT2DM were enrolled in the program.
The sample size was determined based on Power Analysisusing G*Power software sufficient for Repeated MeasureANOVA statistics with statistical power at 0.80, p at 0.05,effect size at 0.33 according to a previous study18 obtaining 23participants. Attrition rate 25% was added, so 30 people withT2DM were enrolled in the program.
The potential participants passing the inclusion criteriawere randomly selected without replacement in the program.However, we lost six participants during the MASE programdue to being referred to the district hospital and these werewithdrawn at the 8th week of the project. Finally, we remainedwith 24 participants in predicting the study outcomes.
Research Instruments
The instruments used in this study were divided into twoparts as follows:
The MASE program for 12-week was developed based ona literature review and Bandura’s perceived self-efficacytheory.17 The program included knowledge, demonstration andreturn demonstration of MASE consisting of warming-up,performing MASE by a little bending of the knees at the thirdMASE performance for 30 mins, and cooling down, MASEassignment at home for 30 mins/day 5 times/week for 12-week,group discussion for 60 mins at the 4th , 8th , and 12th week forsharing experience and solving their exercise problems; andtelephone follow-up approximately 20 mins/time at the 2nd,3rd, 5th, 6th, 7th, 9th ,10th, and 11th week. The content of theprogram was validated by three experts in the fields of nursingand general medicine equal to 1.
The evaluation for data collection was divided into threedomains as follow:
Data collection
The study received approval for ethical considerations fromthe Institutional Review Board (IRB), Faculty of MedicineRamathibodi Hospital, Mahidol University, Thailand (ID10-59-26). Participants received written and verbal explanations,learnt of the objectives, methods, risks, benefits, the right towithdraw from the study at any time throughout the study, andsigned the informed consent form. Data were collected by theresearcher at baseline assessment in the 1st week using thedemographic characteristics, CPG, and body composition,including BMI, visceral fat, and skeletal muscle. Then,participants received the program for twelve weeks and datawere obtained at 8th week and after the program as in the 1stweek (Table 1). The data was kept strictly confidential andoverall data was reported.
Statistical Analyses
Descriptive statistics were used to explain the demographicdata. After study variables passing the assumptions, repeatedmeasure analysis of variance (ANOVA) were used to examinethe differences in the mean of CPG, BMI, visceral fat, andskeletal muscle with a statistically significant p < 0.05.
Twenty-four participants with uncontrolled T2DM werecompletely participated in the MASE program for 12-week. The findings revealed that most participants were females(62.5%) with an average aged = 58.38 ± 8.87 years. Mostparticipants were married (75 %), the highest educationalattainment was primary school (91.7 %), and they worked asa farmer (41.7%) with a monthly family income 7,379.17 ±5,894.35 bath. Mean duration of diabetes was to 6.83 ± 4.97years with comorbidity (70.8%) consisting of hypertension(31.0%) and dyslipidemia (23.52%).
Before receiving the MASE Program, the means of CPG,BMI, and visceral fat were at the high level (156.00 ± 43.01,range = 93-258; 28.15 ± 5.31, range =17.39 - 37.83; 13.17 ±6.62, range = 3-29, respectively); however, mean skeletalmuscle was at the low level (24.47 ± 4.27, range =15.0 - 32.2).After receiving the Program, mean CPG, BMI and visceral fattended to decrease, and skeletal muscle was likely to increase;however, all variables were not statistically significantlydifferent at the least interval (F (2, 46) = 1.80, p > 0.05; F (2,46) = 0.31, p > 0.05; F (2, 46) = 0.32, p > 0.05; F (2, 46) =3.12, p > 0.05, respectively) as shown in Table 2 and Figure 2.
Table 1: Data collection procedure.
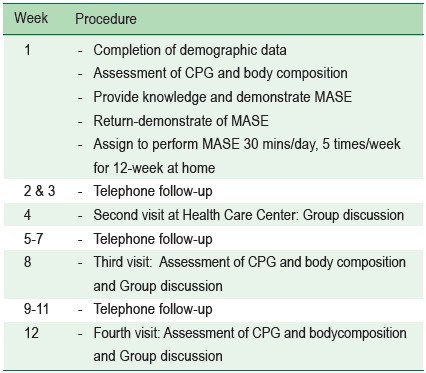
Table 2: Comparison of mean CPG, BMI, visceral fat, and skeletal muscle at the baseline, at the, 8th, and 12th week after receiving the MASE Program using repeated measures analysis of variances (n = 24)
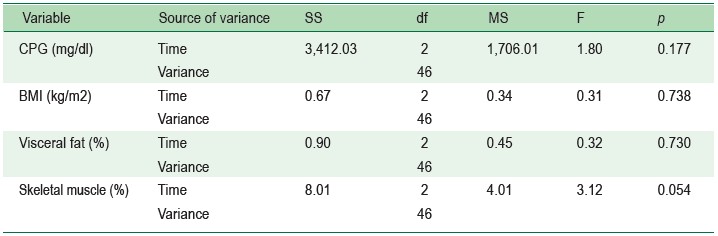
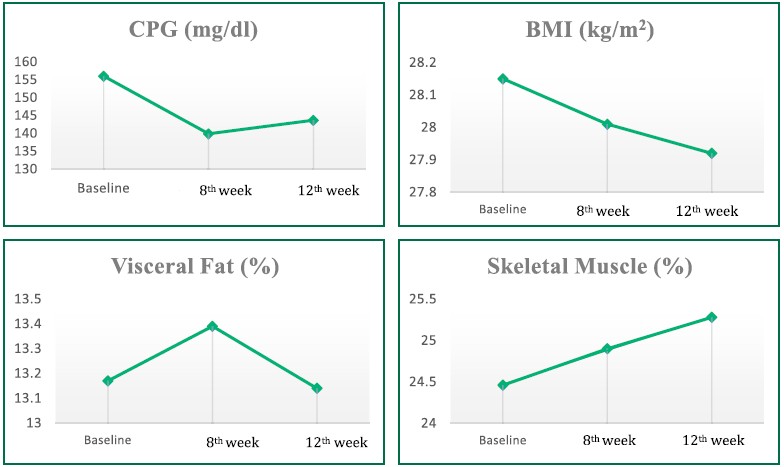
Figure 2: Comparison of mean CPG, BMI, visceral fat, and skeletal muscle at the baseline, at the 8th and 12th weekafter receiving the MASE Program
The results showed that mean of CPG, BMI, and visceralfat have a tendency to decrease, and skeletal muscle showeda slight increase; however, after finishing the program, allvariables were not a statistically significantly different. Thesefindings were different from hypothesis outcomes, althoughparticipants continuously performed the MASE programintegrating Bandura’s Self-efficacy theory using fourresources: mastery experience, vicarious experience, verbalpersuasion, and physiological and effective states.17 Unfortunately,approximately half of the participants in this study (41.7%)were older adults with a low level of skeletal muscle, and averageBMI and visceral fat were at a high level resulting in insulininactivity and insulin resistance leading to effectively decreasein glucose uptake in skeletal muscles.19,20,21 Besides, the highlevel of visceral fat, especially around the abdomen, suppressionof glucose transporter 4 (GLUT-4) resulted in high bloodsugar. Therefore, achieving glycemic control in this study couldbe more difficult than in younger people with diabetes anda normal BMI.22
Moreover, visceral fat is determined as a major factorassociated with the development of inflammation, vasculardysfunction, and atherosclerosis in the human body.5 Excessivevisceral fat can also strengthen inhibition of skeletal muscleglucose uptake23 and insulin resistance leading to difficulty forcontrolling the disease.24 The results in this study werecontrasted to a previous study using TASE finding a significantdecrease in HbA1C and BMI.13,14 Possibly, the participants inboth studies had more activities and lower BMI than participants
This study can be generalizable to people with uncontrolledT2DM being similar characteristics of the sample. However,the study lacks a control group. Thus, further study should usea randomized control trial to examine the effects of the MASEProgram for a period of at least 6 months, especially in olderadults who are overweight.
Based on these results, the MASE Program should berecommended to people with uncontrolled T2DM for morethan 12 weeks since the outcomes are better than before theProgram.
The authors declare that they have no conflicts of interest









