Electronic ISSN 2287-0237
Asbestos exposure is the most common risk factor of mesothelioma. Asbestos is a group of fibrous silicate minerals that occurs naturally. These minerals are found in soil and rocks in many parts of the world. The links to MM associated with asbestos exposure as a common cause of MM, accounted for 80-90% of cases.1,3,4,7,8 The incidence level depends on the amount of fiber and the length of time of exposure to asbestos.9
Zeolite fiber is a fibrous mineral and its structure is chemically similar to asbestos. It has also been reported to cause MM in animal and human studies.
There have been a few published reports of MM developing after exposure to radiation. In these cases, patients had been exposed to high doses of radiation to the abdomen or chest as treatment for another cancer. However, the cumulative incidence of MM after a-40-year exposure to radiation was very low.10,11
The simian virus 40 (SV40) is a DNA virus that was isolated in 1960 from contaminated polio vaccines.12 Many studies demonstrated that SV40 induced MM in hamsters13 and humans.12,14 Moreover, some studies showed that the SV40 virus was a cofactor with asbestos fibers in the development of MM in animal models and in humans.
MM can be found in several areas in the body15,16
1. Pleural mesothelioma is the most common type of mesothelioma and accounts for 90% of all mesothelioma diagnoses.17,18 Symptom and signs of patient with pleural mesothelioma are nonspecific include chest pain, cough, shortness of breath, pleural effusion, hemoptysis etc. The diagnosis often occurs at an advanced stage. If patients are left untreated, the survival rate is less than one year.7
2. Peritoneal mesothelioma is less common than pleural mesothelioma and accounts for approximately 4.5% of mesothelioma diagnoses.2 Peritoneal mesothelioma presents with abdominal pain, ascites, weight loss, and bowel dysfunction. However, signs and symptoms of peritoneal mesothelioma only occur at a later stage.
3. Pericardial mesothelioma is rare a malignancy occurring at a rate of 0.0022% in a series of nearly 500,000 random autopsies.19-21 Symptoms and signs of pericardial mesotheliomas are nonspecific include pericarditis, heart failure, pulmonary embolism, and cardiac tamponade etc. Finally diagnosis is usually made after surgery or at autopsy.19 (Figure 1)
4. Mesothelioma of the tunica vaginalis, is an extremely rare tumor, and consequently very little is known about the clinicopathological spectrum of this variant as a distinct entity.22,23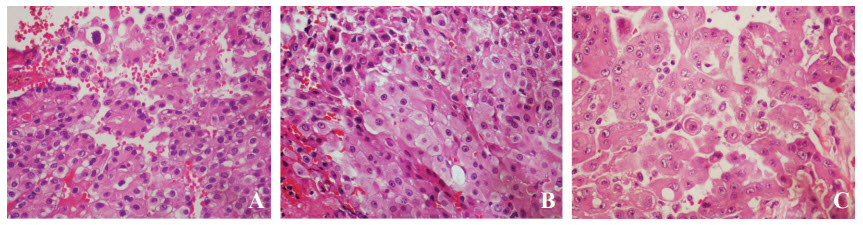
Figure 1: An example of peritoneal malignant mesothelioma is shown. Hematoxylin and eosin-stained sections demonstrate papillae (A) and sheets (B) of tumor cells. They have oval-shaped vesicular nuclei, visible nucleoli, and voluminous pale eosinophilic cytoplasm (C). Case courtesy of Prof. Shanop Shuangshoti, MD
MM can be classified in 3 main histologic cell types.24,25
2. Sarcomatoid MM: This cell type has the worst prognosis and is resistant to both chemotherapy and radiation therapy.
3. Biphasic MM: This cell type is composed of epitheloid and sarcomatoid cells. Biphasic cell type has an intermediate response to chemotherapy and radiation therapy.
Biomarkers may be helpful in the diagnosis of MM. These biomarkers include:26
1. Serum biomarkers for MM:
- Soluble mesothelin-related protein (SMRP)
- Mesothelin/ERC
- Osteopontin (OPN) or bone sialoprotein I (BSP-1 or BNSP)
- Fibulin-3 Soluble syndecan-1
- Circulating fibrinogen
- RANTES/CCL5 (chemokine (C-C motif) ligand 5)
- Hyaluronan/hyaluronic acid
- YKL-40/chitinase-3-like-1
2. Biomarkers for MM in pleural effusion: among the above-mentioned biomarkers, MRP, fibulin-3, N-ERC/mesothelin, hyaluronic acid and OPN are used for early diagnostic biomarkers of MM.
3. Immunological alterations caused by asbestos exposure and their use as biomarkers for MM such as CXCR3 (Chemokine (C-X-C motif) receptor 3X), interferon(IFN)-γ, and NKp46 on the cell surface of Natural killer (NK) cells etc.
I) Surgery
Surgery is an invasive method used to remove a mesothelioma tumor. The percentage of success depends largely on the stage of malignancy and degree of organ involvement. In 2008, a significantly large study showed that the median rate of survival with surgery (including extrapleural pneumonectomy) was 11.7 months only. However, the data indicates varied success when surgery was perform in combination with chemotherapy and radiation therapy.27
II) Radiation
Radiotherapy is a common method of treatment applied to the sites of malignancy. The radiation can be given pre-operatively to reduce the size of the tumor and post-operatively in order to prevent tumor re-growth and recurrence of new tumors.
III) Chemotherapy
The guidelines recommend the use of combination therapy, but monotherapy can be used in patients who are unable to tolerate more than one drug, chemotherapy include;
- Antifolates
Antifolate agents were among the first chemotherapy agents to demonstrate significant activity in mesothelioma. In February 2004, the Food and Drug Administration approved pemetrexed used alone or in combination with other medication in the treatment of pleural mesothelioma. The mechanism of pemetrexed is that it inhibits 3 enzymes in purine and pyrimidine synthesis: thymidylate synthase, dihydrofolate reductase, and glycinamide ribonucleotide formyltransferase. Administration of high-dose methotrexate (3 g/m2 every 10-21days) with leucovorin was associated with a response in 22 of 60 patients (37%), with a median survival of 11 months.24,28
- Gemcitabine
Gemcitabine (2’,2’-difluoro 2’-deoxycytidine, dFdC) is the most important cytidine analogue developed since cytosine arabinoside (Ara-C). Gemcitabine can used in various malignancies such as non-small cell lung cancer, pancreatic cancer, bladder cancer, breast cancer, and it shows activity in the treatment of mesothelioma. The evidence of anticancer activity of gemcitabine is evident in a wide spectrum of in vitro and in vivo models and has also been successfully confirmed in the clinical setting.29,30 Gemcitabine is only administered intravenously, since it is extensively metabolized by the gastrointestinal tract.
- Vinorelbine
Vinorelbine (Navelbine®) is a semisynthetic of vinca alkaloid, and also has demonstrated activity against mesothelioma. The mechanism of action is the inhibition of mitosis through interaction with tubulin leading to apoptosis. The mechanism of the mitotic block is unknown.31 Vinorelbine is administered either orally or intravenously. In previously untreated patients with mesothelioma, the combination of cisplatin plus vinorelbine was associated with a response rate of 30%. These results are reasonably similar to those achieved with platinum-based doublets that include pemetrexed or gemcitabine.24
- Anthracyclines
Anthracyclines, include doxorubicin and idarubicin, remain an important class of chemotherapeutic agents derived from Streptomyces bacterium and Streptomyces peucetiusvar caesius.32 In clinical trials of single-agent treatment with doxorubicin or epirubicin, the result show poor response rates was range from 0% to 15%.24
IV) Targeted Therapies
- Angiogenesis Inhibition
Vascular endothelial growth factor (VEGF) inhibitor is a substance that inhibits the formation of new blood capillaries (angiogenesis) from preexisting vessels. VEGF inhibitor has a potential role acting as an antiangiogenic agent in mesothelioma. VEGF inhibitor can be used in MM such as Bevacizumab, Vatalanib, Sorafenib etc.
- Epidermal Growth Factor Receptor Inhibition
Epidermal growth factor receptor (EGFR) is expressed in approximately 68%-96% of mesothelioma cells. Moreover, treatment of mesothelioma cell lines derived from previously administered Gefitinib, has resulted in the inhibition of EGFRdependent cell signaling and also dose-dependent reduction of tumor formation.24
- Other Agents24,34,35
a. Histone deacetylase inhibition such as Vorinostat (in a phase I trial)
b. Ribonucleases such as Ranpirnase (in a second phase III trial)
c. Morab-009 is a monoclonal anti-mesothelin antibody.
d. SS1P is an anti-mesothelin antibody with a conjugated toxin (Pseudomonas exotoxin type A)
e. CRS-207 is a mesothelin vaccine derived from attenuated Listeria monocytogenes.
Although MM is a rare cancer, its incidence is still increasing. The aggressive nature of MM which responds poorly to treatment leads to a grave prognosis. Early detection and treatment with a combination of surgery, chemotherapy, and radiation therapy improves survival rate. Targeted therapy may become the new choice of treatment in the future.









