Electronic ISSN 2287-0237
Metal on Polyethylene bearings have been widely used in total hip replacements for over 40 years. However there are still concerns about implant failures due to aseptic loosening and osteolysis, which occurs as a result of immune system responses triggered by the microscopic debris generated by normal wear and tear of the prosthetic joint.
Willert1 suggest that Ultra-high monolecular weight polyethylene (UHMWPE) can be responsible for the formation of osteolysis occurring in areas around endoprosthetic implants, especially if greater amounts of this polymer’s particles are released into the tissue.
In 1992, Amstutz et al.2 discussed the factors leading to massive osteolysis, namely polyethylene wear debris induced osteolysis. Macrophages activated by phagocytosis of particulate wear debris are the key cells in this process. (Figure 1)
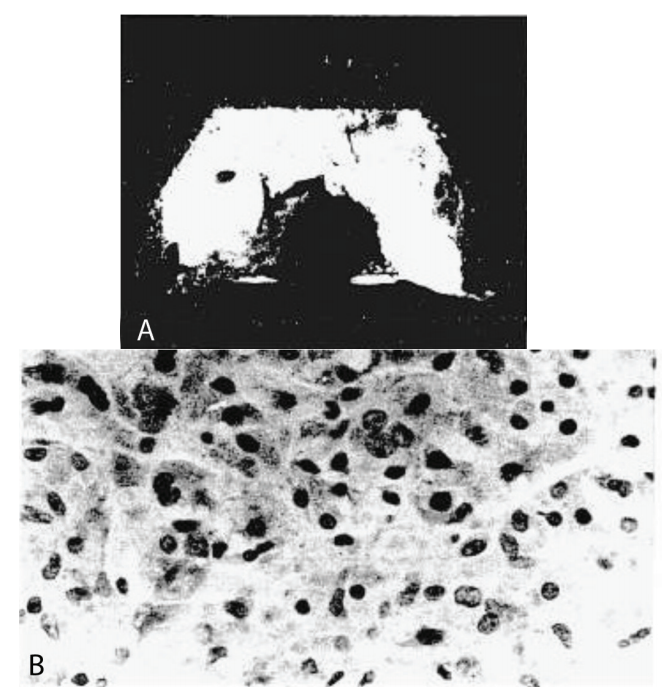
Figure 1 A-B: (A) Retrieved titanium-alloy femoral porous-coated surface replacement bisected to show the replacement of bone by an invasive granulamalike tissue. This component failed after 50 months in an active 62-year-old man. (B) Histology of the tissue within the femoral head shows sheets of macrophages and giant cells, many with fine, intracellular metallic or UHMWPE debris. Lymphocytes are rarely seen in theses tissues. (Stain, toloidine blue; original magnification, X60.)
Therefore, due to the most common cause of implant failure in Total Hip Replacement still being aseptic loosening from polyethylene wear debris, new bearing surfaces have been developed, such as ceramic on ceramic, in an attempt to reduce wear debris
Hard on Hard bearings (Ceramic on ceramic (COC) and Metal on metal) were developed because the long term outcome of Metal on non cross linked polyethylene was unsatisfactory due to the aforementioned extensive osteolysis from macrophage induced osteolysis.2 Historically, the use of ceramic bearing was first introduced in April 1970 with Alumina-on-alumina bearings by Dr. Pierre Boutin3 (Figure 2).
The advantage of ceramic on ceramic (COC) was shown by in vitro analysis to reduce wear debris particles that cause osteolysis4,5 and Ceramic bearings made from Alumina have showed the lowest in vivo wear rates of any bearing couples.6 The important property of ceramic that caused a lower wear rate was its being hydrophilic (Figure 3) Ceramic’s hydrophilic properties facilitate an increased wettability of the surface because of the strong hydrogen bonds between the ceramic surface and synovial fluid that results in the synovial film being more uniformly distributed. In addition, ceramic has a greater hardness than metal and can be polished to a lower surface roughness (Figure 4). Lastly, ceramics have a high degree of Biocompatibility. Catelas et al.7 reported in vitro studies show less macrophage reaction and decreased cytokine secretion when exposed to ceramic particles versus high-density polyethylene because of their small size, low volume, and inertness. These overall properties of ceramic create the lowest coefficient of friction and this bearings combination is the most likely to achieve true fluid film lubrication.8
Figure 2: Dr. Pierre Boutin (photograph courtesy of Laurent Sedel, MD)
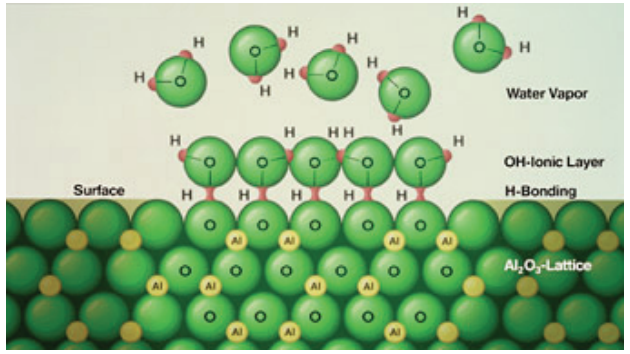
Figure 3: The strong hydrogen bond that forms between ceramic surfaces and synovial fluid give ceramic materials wetting properties that are superior to those of metal and polyethylene.
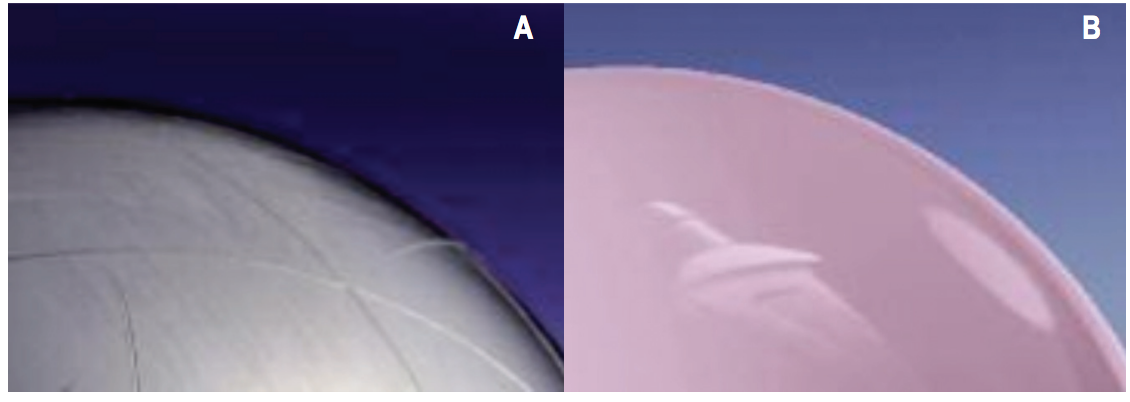
Figure 4 A-B: Shows no scratches on fourth Generation ceramics surface due to high degree of Hardness. (A) Scratched surface increases abrasion on surface of cup liners made of Polyethylene And Metal (CeramTec). (B) Only an unscratched smooth surface of the sort achieved in Fourth Generation ceramics enables optimal wetting, outstanding lubrication and minimal wear (CeramTec)
However, the results of the early generation of COC were not promising due to poor design, inadequate material properties, and imperfect craftsmanship leading to catastrophic failures with ceramic fractures and excessive wear rate.
The first generations of COC were introduced between 1974 and 1988; at that time long sintering times resulted in large grained size material, which lead to decreased strength and crack propagation and thus a high incidence of ceramic fracture. The second generation of COC was developed between 1988 to 1994. Mixing micro-arc oxidation (CAO) and magnesium oxide (MgO) as sintering aids into the Alumina also limited the grain size, thus decreasing incidence of ceramic fracture. The Third Generation of COC was developed between 1994 to 2004. Improvements in manufacturing such as isostatic pressing, laser etching and proof testing resulted in a purer, denser ceramic with a small grain size, which reduced crack propagation and fracture.9
The mechanical properties of the three generations of ceramics are summarized in Table 1.8
The newest or fourth generation ceramic on ceramic design is Alumina-Matrix-Composite (AMC) or BioloxDelta (Figure 5) which is composed of Alumina Oxide (approximately 75%), Zirconium Oxide, Chromium Oxide and other oxides. The combination of mechanical properties (fracture strength of Zirconia ceramic is approximately double that of alumina) and the good tribological properties of alumina ceramic make this an improved material for hip implants.
Alumina Ceramics
Ceramics can be defined as inorganic non metallic materials compounded of a non metal and a metal. Alumina is a monophasic polycrystalline, very hard, stable and highly oxidized, with a high thermal conductivity coefficient, low bending stress and low resilience. The resultant material is in its highest state of oxidation, allowing thermodynamic stability, chemical inertness, and therefore excellent resistance to corrosion. The ionic structure of alumina ceramic creates a hydrophilic structure and fluid-film lubrication resulting in a higher wettability. In vitro studies show water is absorbed with high bond strength and that proteins quickly and completely cover the ceramic surface with a monolayer after surgical implantation; this phenomenon therefore improves lubrication of the joint. But Alumina ceramics are brittle because of excellent compression strength and bending strength is limited. Alumina ceramics can also break without warning signs due to low fracture toughness: ceramic has no possibility to deform without breakage.11
Table 1: The Changes in Grain Size and Burst Strength for Each Generation of Ceramic Manufacturing

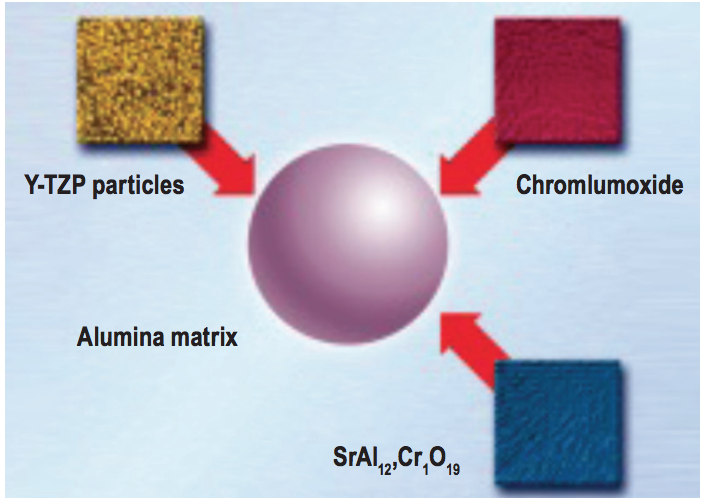
Figure 5: Composition of the alumina matrix composite (CeramTec)
Zirconia
Ceramic Zirconia was introduced due to its higher fracture toughness and bending strength. However, pure zirconia is an unstable material exhibiting three crystalline phases: monoclinic, tetragonal, and cubic. The change between the three phases results in large volume changes and decreases the mechanical properties of the material considerably because of cracking on cooling. Adding oxides during the tetragonal phase stabilizes zirconia. Yttriumstabilized tetragonal polycrystalline zirconia (Y-TZP) has a fine grain size and offers the best mechanical properties. The tetragonal phase that is the most resistant tends to transform into the monoclinic phase. This phenomenon explains the higher resistance of zirconia to shock but it also explains its lower sliding resistance properties and its unstable situation over time.11 Another concern with Y-TZP is its hydrothermal stability. Because Y-TZP is destabilized during the process of steaming sterilization (causing surface roughness of zirconia due to hydrothermal transformation) these ceramics may also undergo slow degradation during long term implantation in the human body. This low temperature degradation is only significant after several years, but can still call the use of zirconia-onzirconia bearings systems into question.12
Because of the brittleness of Pure Alumina ceramics and hydrothermal instability of Zirconia, it would seem that a composite of these materials with better mechanical properties would be the way to improve reliability of ceramics implants in orthopedics. De Aza et al.13 studied crack growth resistance, comparing between 3 types of ceramics: alumina, zirconia and alumina-zirconia composite. They concluded that alumina-zirconia composites have a higher reliability than the monolithics due to the combined advantages of both alumina and zirconia. Alumina-zirconia nanocomposites with relative low zirconia content present similar hardness values to alumina but are not susceptible to hydrothermal instability.
Ceramics are extremely hard, making them wear and scratch resistant however this also indicates a relatively high degree of brittleness, which led to failures in earlier designs. The new Ceramic design Alumina-MatrixComposite has extremely high fracture toughness and is resistant to crack propagation results as the result of two strengthening mechanisms.
1. Airbag Function
The first toughening mechanism is dispersion of nano-sized, yttria-stabilized tetragonal zirconia particles in a stable, alumina matrix. These particles will be homogenously distributed and produce local pressure peaks in the area of crack which counteracts crack propagation and works like the airbag system in cars. (Figure 6)
2. Counteracting Crack Formation
The second strengthening mechanism is the result of in situ formation of platelet-shaped crystals in the oxide mixture. These platelets prevent cracking and crack propagation by deflecting the crack path and neutralizing crack energy. (Figure 7)
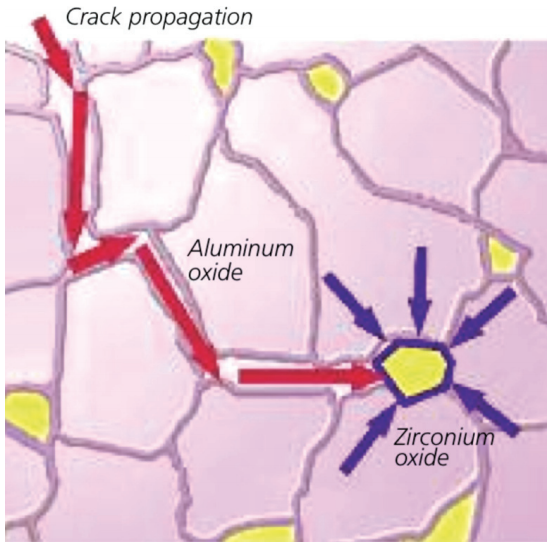
Figure 6: The principle of conversion reinforcement: Zirconium oxide particles act like airbags by absorbing impacting forces. (CeramTec)
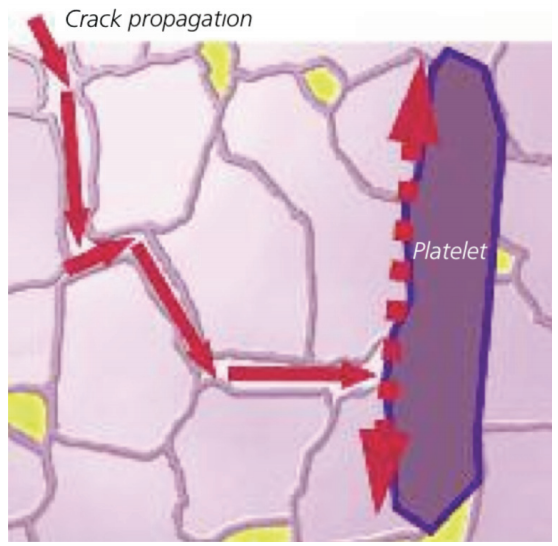
Figure 7: The principle of platelet reinforcement: Platelet-shaped crystals block the propagation of cracks and thereby increase overall strength.
1. Squeaking Sounds
After improvements in ceramic manufacturing, the incidence of ceramic fracture decreased especially after third generation of ceramics. Over the last 5 years, the orthopedic community has been concerned with the noise of ceramic bearings, which was well documented with incidence varying from 1%-20.9%.14-16 The squeaking noise was defined as a high-pitched noise audible to the human ear.
This disturbing, squeaking sound is like the sound of a new pair of shoes during walking and it annoys and worries patients. Mostly sound occurs during mid range of motion while weight bearing as in simulated stair climb.
The ten year follow up study by Chevillotte et al.17 reported 100 Total hip replacements implanted with COC during November 1999 - December 2000; all hips used third generation ceramics (Biolox Forte, CeramTec). To determine the causes and consequences of squeaking, the patients were evaluated by questionnaire. Five patients (five Hips) reported the squeaking sound. The squeaking noise appeared at a mean of 66 months (4 to 85 months) post surgery with an incidence 2.2% at ten year follow up. The result showed more frequent squeaking sound found in hips in heavier (p < 0.0008) and taller males (p < 0.0001) and these result are in agreement with Walter18 and Poggie.19 Nevertheless, after 10 years of follow-up, patients with squeaking hip did not have any excessive wear, head fracture, cup or stem loosening, abnormal pain, or any limitation of their activities. Harris hip score and Postel-Merle d’Aubigné score were comparable. Squeaking did not disappear in the time but remained stable in intensity. Radiographic assessment did not found malpositioning of the cup in squeaking hips. They concluded that squeaking noise seem to be an isolated phenomenon with no consequence for functional result on longevity at ten years follow up.
In 2009, Chevillote et al.20 reported a biomechanical in vitro study of COC bearings surface which intended to identify the potential contributing factors of Hip Squeaking. They used a custom-made hip stimulator to assess in vitro hip squeaking (Figure 8, 9). All Acetabulum Components were positioned in 45 degrees abduction and 20 degrees of anteversion. Eight conditions in two separate situations were applied to testing(Table 2 and Table 3).
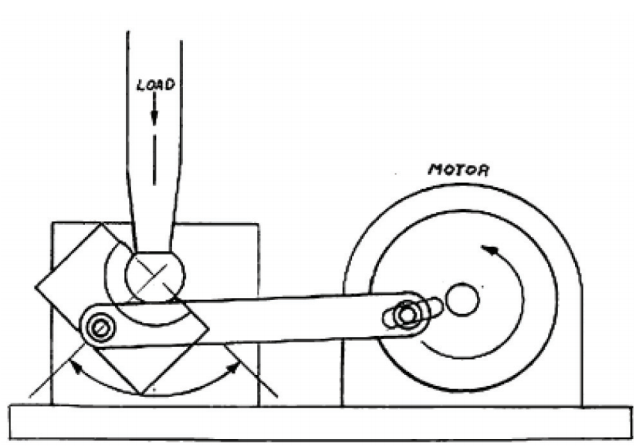
Figure 8: A diagram of the custom-made testing device hip simulator
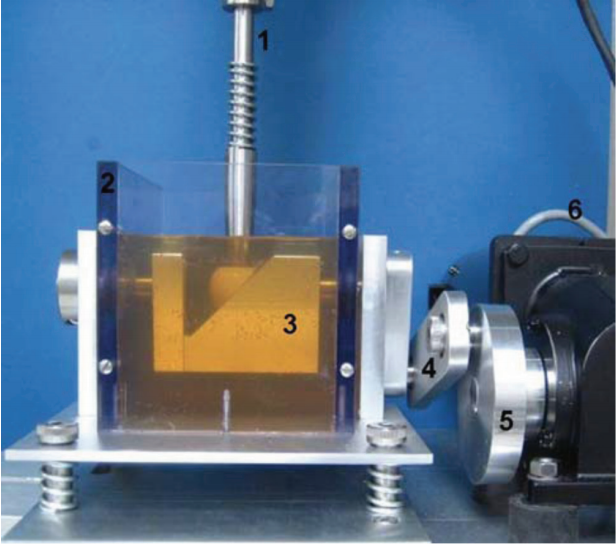
Figure 9: A photograph of the custom-made device is shown. 1 = Servo hydraulic testing machine 2 = box 3 = rotating table 4 = bar linkage 5 = rotating jig 6 = motor
Table 2: Situation without lubrication.
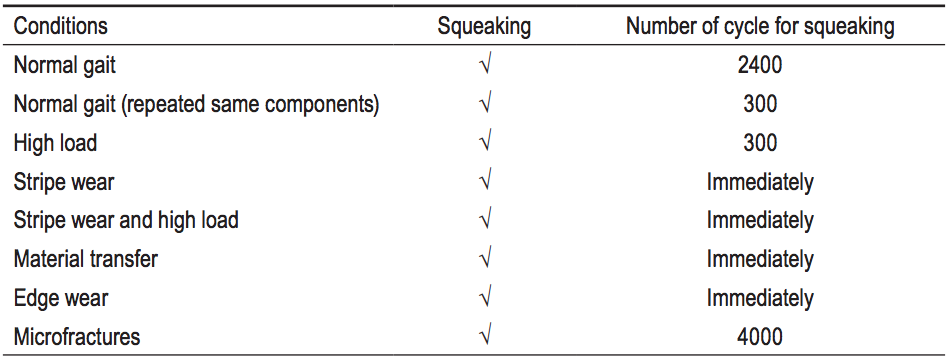
Table 3: Situation with lubrication
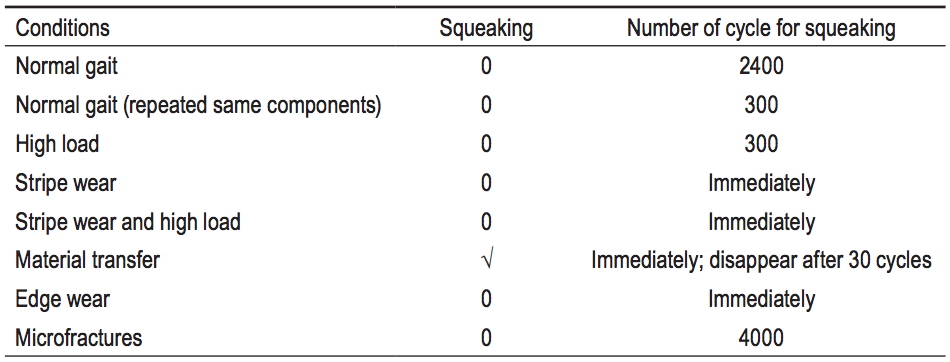
Table 2’s results show the squeaking sound was easily reproducible in all dry conditions, the squeaking noise was constant and did not disappear with time. In all these dry conditions, when a small amount of lubricant was added, the squeaking sound would disappear but if the lubricant was stopped, the squeaking would reappear and remain. Comparative to lubricated conditions, noise occurred only in material transfer condition (interposed of metal particles between head and liner). This suggested the exact etiology of squeaking is a disruption of fluid lubrication and this phenomenon occurs when the film fluid between the two surfaces in contact is disrupted. The researchers suggested this interruption most commonly results from metal particle transfer as a third body between COC.
Respeto et al.21 reported the metal debris and stripe wear in four COC total hip replacements after revision surgery due to problems from squeaking noise.
Walter et al.22 found bands of stripe wear in many ceramic heads after revision surgery without any previous squeaking problem So, in the conditions where there is a high risk to generate metal wear debris in COC hip replacement (such as neck rim impingement, malpostioning of acetabulum components, short neck design stem or some design of acetabular component with metal rim around the edge) the debris can interrupt the fluid film lubrication in COC Hip Replacement, resulting in squeaking noise. For the prevention of this disrupting sound the surgeon should pay attention to cup orientation and select the proper design of femoral stem and acetabulum cup.
2. Stripe wear
Stripe wear is the term used to describe the long, narrow area of damage seen on some femoral heads retrieved from alumina COC hip bearing couples. Stripe wear has been reported in first and second generation alumina bearings23 However, there were also reports of stripe wear in third-generation alumina ceramic-on-ceramic bearings with well fixed and well positioned acetabular components.24 (Figure 10)
Some literature reported produce stripe wear was due to edge effects in rigid ceramic-on-ceramic total hip arthoplasty.26-28 When the hip was slightly subluxated during the swing phase of gait, the cup edge might create an inferior and somewhat equatorial stripe on the femoral head along with a circumferential stripe along the cup rim. During forced reduction at heel-strike, a superior and somewhat equatorial stripe would then be created on the head and the mating cup rim.19(Figure 11).

Figure 10: Third generation alumina ceramic- on- ceramic bearings with well fixed and well positioned acetabular components
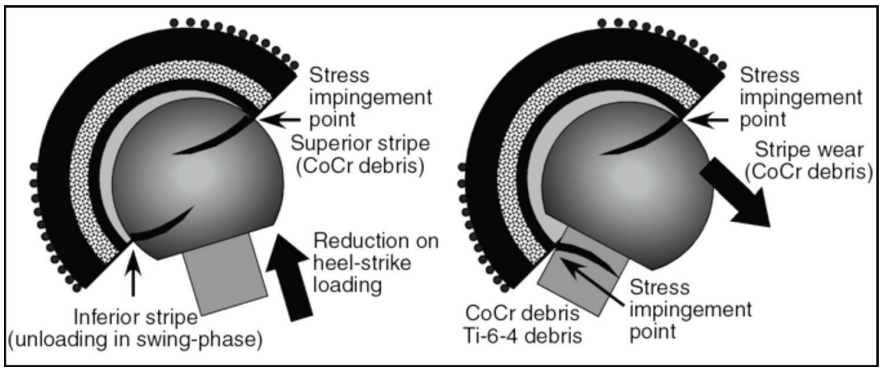
Figure 11: During forced reduction at heel-strike, a superior and somewhat equatorial stripe would then be created on the head and the mating cup rim
Nevelos et al.30 proposed that microseparation of the bearing centers occurs during the swing phase of normal walking and that the subsequent edge loading with heel strike causes the stripe.
In an analysis of 16 retrieved third generation alumina COC bearings, the reseacher proposed that stripe wear was caused by edge loading between acetabular liner and femoral head ceramic component.31 The pattern of wear stripes on the heads and liners showed that the majority do not occur with normal walking; instead they probably occur with edge loading when the hip is flexed such as in rising from a chair or climbing a high step. The mean volumetric wear rates of COC bearings in that study were 0.7 mm3 per year (running-in). For the effect of alumina ceramic wear, in vitro study on the biologic activity of ceramic particles suggests that they will not be more destructive than polyethylene particles.32
The wear particles produced by alumina ceramic on-ceramic bearings are not in the correct size range (0.1–1 micrometer) to stimulate macrophages to produce TNF. For this reason, volume of wear debris from stripe wear will neither be related to osteolysis nor to bearing failure.31
Total hip arthroplasty is often a successful orthopaedic surgical procedure. To improve longevity of prosthesis, many alternative bearings have been explored. One attractive choice is alumina ceramic-on-alumina bearings due to its properties of low friction, high wear resistance, and good biocompatibility. On the other hand, ceramic on ceramic bearings have problems of fracture of a ceramic head and/or liner. Many attempts were made to improve alumina material, that was associated with high rates of fracture as reported in the 1970s (Table 4).32,33
Table 4: Summary of the mechanical properties of the material used in ceramic-on-ceramic bearings over the past 40 years
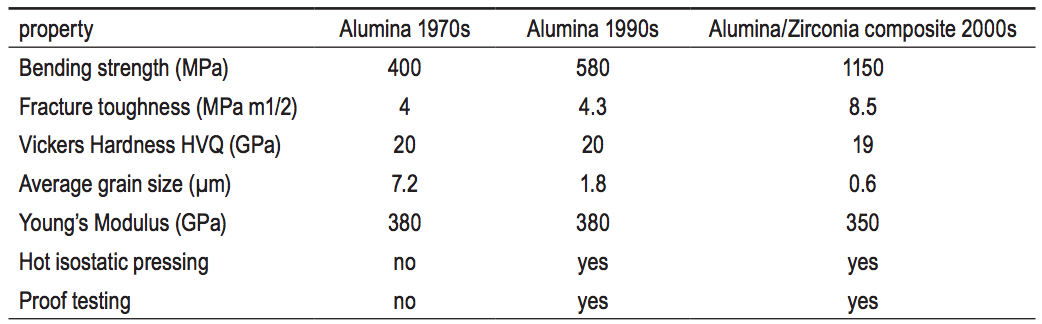
Improvements of second-generation ceramics included purification of alumina powder, leading to smaller grain size. This, along with refined manufacturing, increased the density, resulting in decreased fracture rates to 0.014%.34-36 Third generation fracture rates were reduced to 0.004%.34-36 In the 2000s, the introduction of alumina/ zirconia composite materials showed improvement in mechanical properties For this reason, the reported incidence of alumina femoral head fractures has decreased. The rate of fracture of femoral heads with this material is reported by the manufacturer to be 1 in 50,000.37 In 2010, Lombardi et al.38 reported atraumatic fracture of AMC femoral head. The analysis of the fractured alumina matrix composite femoral head demonstrated the surface roughness increased minimally from new condition (3 nm) to the main wear zone (5 nm) (Figure 12, 13).
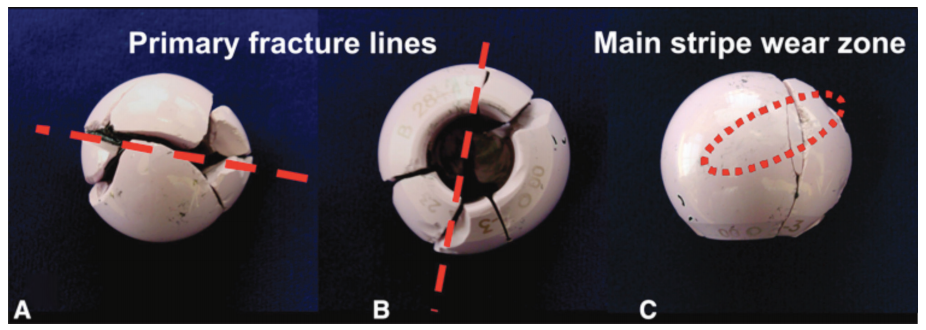
Figure 12A-C: Overview of fracture fragment from a 28-mm delta from (A) polar view, (B) view of the base, and (C) side view of the stripe wear zone. The dominant fracture plane is indicated by dashed lines in the polar and basal views. The large stripe wear zone crosses over three of the fragments at the angle indicated by the dashed ellipse on the side view
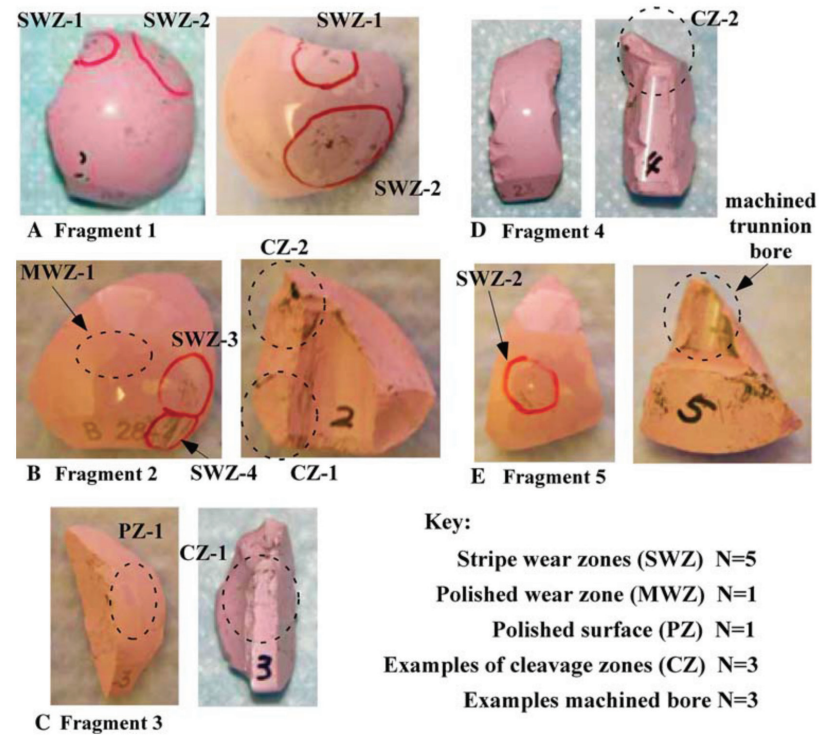
Figure 13A-E: Photographs show five of the largest of seven fragments (A-E) from a fractured 28 mm ‘Delta’ ball. The circles indicate site of analysis for polished main wear zone (MWZ), stripe wear zones (SWZ), metal contamination, machined taper bore and fracture cleavage regions (CZ).
Hamilton et al.39 also reported the overall rate of postoperative ceramic liner fracture was 1.1% (two of 177). The authors presumes most liners failed as a result of eccentric or incomplete seating of the modular ceramic liner within the metal acetabular shell. Improper positioning and impaction may generate uncontrolled peak stresses in the ceramic, which may lead to fracture40 (Figure 14).
Many predisposing factors for ceramic liner fracture were proposed such as microseparation trauma, and Figure 12A-C: Overview of fracture fragment from a 28-mm delta from (A) polar view, (B) view of the base, and (C) side view of the stripe wear zone. The dominant fracture plane is indicated by dashed lines in the polar and basal views. The large stripe wear zone crosses over three of the fragments at the angle indicated by the dashed ellipse on the side view Figure 13A-E: Photographs show five of the largest of seven fragments (A-E) from a fractured 28 mm ‘Delta’ ball. The circles indicate site of analysis for polished main wear zone (MWZ), stripe wear zones (SWZ), metal contamination, machined taper bore and fracture cleavage regions (CZ). obesity.41-43 Fractures apparently due to component impingement were explored.40,44-46 There were reports that ceramics are vulnerable to fracture due to impact and from stress concentrations (point and line loading) such as those associated with impingement-subluxation.47 The risk of ceramic femoral head fracture during impingement-subluxation was found to be highly site specific owing to the greatly higher tensile stress at the (edge-loading) egress site compared with that from neck-on-liner impingement (Figure 15).
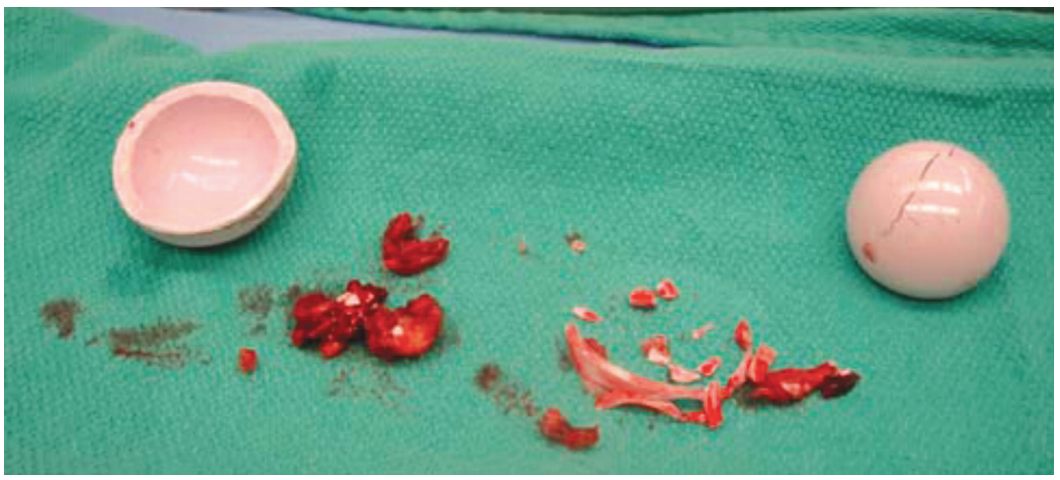
Figure 14: The retrieved liner and head show the fractured rim of the liner and ceramic fragments retrieved from the wound.
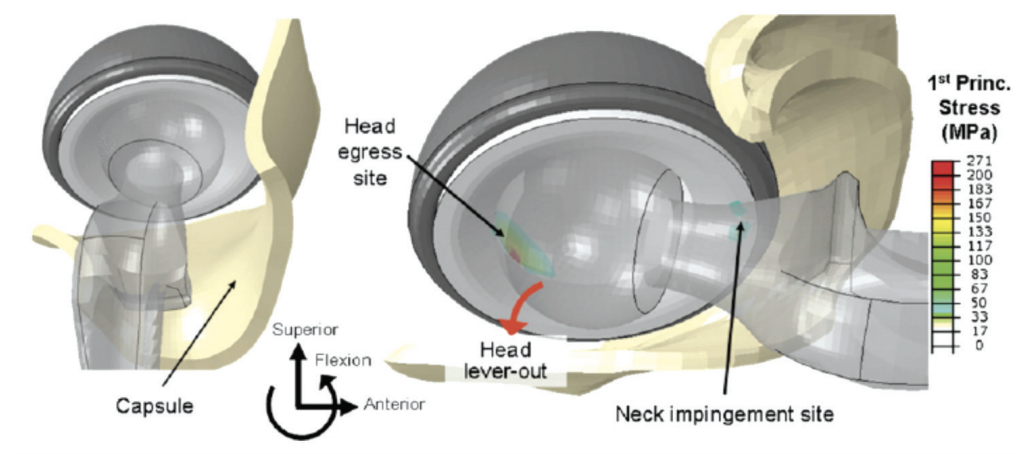
Figure 15: Total hip arthoplasty impingement global FE model. Challenge motions began in full extension (left) and progressed through the prescribed hip angulation sequence, resulting in impingement (right).
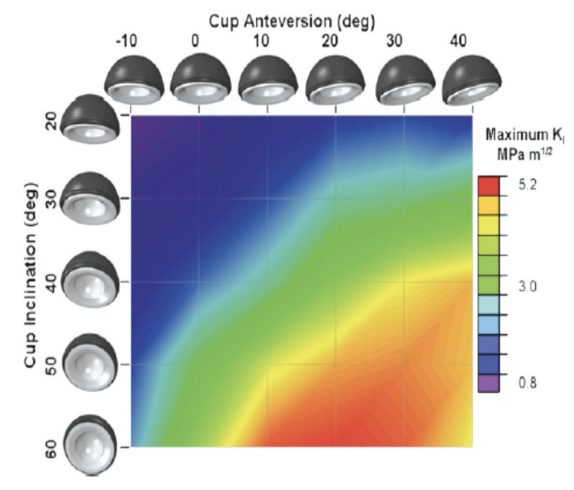
Figure 16: Computed values of temporal-spatal maximum KI for the stoop challenge demonstrating fracture propensity sensitivity to both cup inclination and anteversion.
Another interesting factor is cup position. The biomechanic study showed ceramic cup fracture propensity is presumably very sensitive to surgical cup positioning. Higher cup inclination and/ or cup anteversion angles gave rise to the higher values of tensile stress if/when subluxation-associated edge loading occurred (Figure 16). The study of the stress on cup position concluded that increased cup inclination and increased anteversion were found to elevate fracture risk. It is resonable to avoid impingement-subluxation, higher cup inclination and cup anteversion of ceramic bearing to reduce risk of ceramic bearing fracture.
The tribology properties of low friction, high wear resistance and good biocompatibility make ceramic material the most attractive in hip replacement surgery at the present time. In long term follow up after implantation, the ceramic couple bearings show the lowest wear rate in many reports, which means low wear debris and less osteolysis.
Specific concerns about ceramics such as fracture, squeaking noise, and stripe wear are still topics of discussion among orthopedic surgeons. Significant advancements in manufacturing processes led to the production of alumina matrix composite ceramics that could eliminate the previous ceramics weaknesses. As for surgical factors, surgeons should perform operations with meticulous technique especially during positioning of the acetabulum component, and insertion of ceramics liner, and they check for any impingement or infolding of anterior-superior capsule, and check the hip tension to prevent hip laxity. These factors can all reduce complications from ceramic implants.
Otherwise, due to the continued high cost of ceramics implant (about double that of metal on polyethylene) it is suggested that good candidates for ceramics implants should be young, active, high demand patients that will need to use their new hip joints long term.









