Electronic ISSN 2287-0237
To study the accuracy of the 256 Multi-detector Computerized Tomography (MDCT) in detecting coronary artery stenosis.
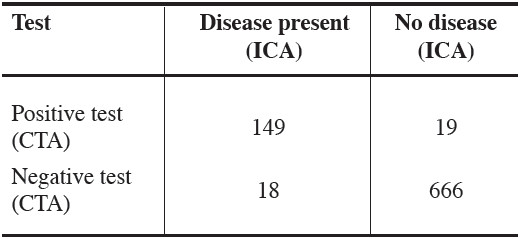
We retrospectively analyzed angiographic findings of patients who underwent both 256 MDCT and invasive coronary angiography (ICA). All epicardial arteries, regardless of calcium burden, were segmented into proximal, mid and distal part for comparative analysis. Significant coronary artery stenosis was defined as the reduction of luminal diameter being equal to or more than 50%. The diagnostic accuracy of 256 MDCT in coronary artery stenosis evaluation was assessed by comparing its’ sensitivity, specificity, positive and negative predictive values to the gold standard ICA.
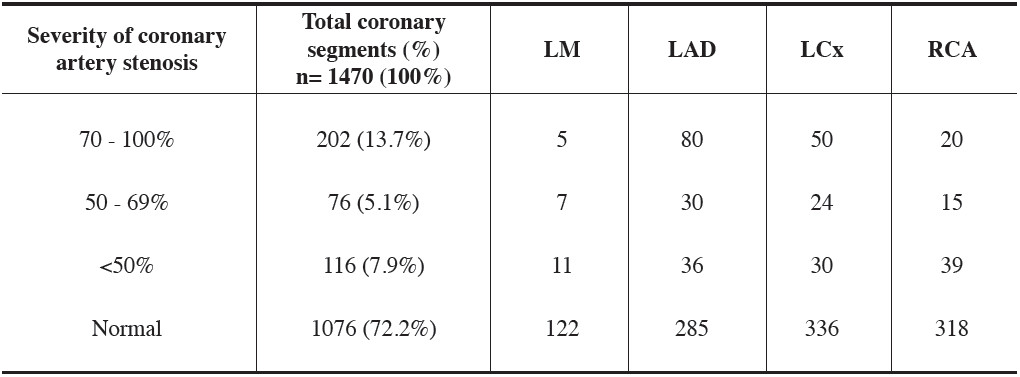
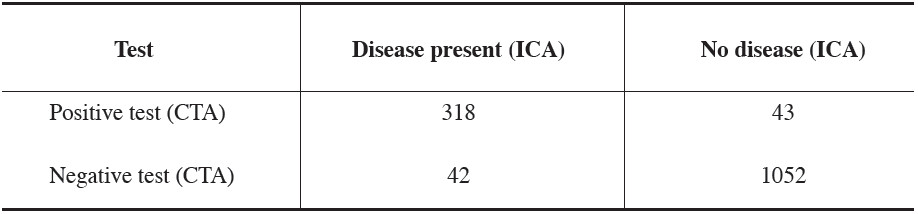
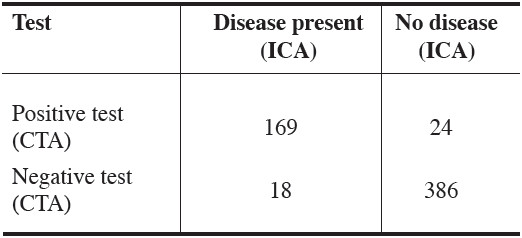
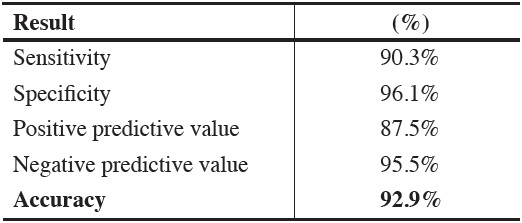
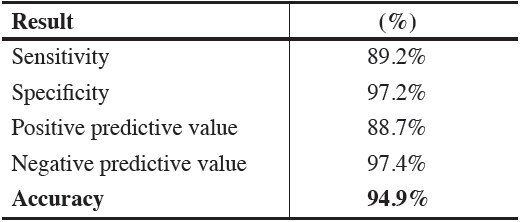
From January to December 2009, a total of 147 consecutive patients (124 male, 23 female, mean age of 60 ±12 years) underwent both MDCT and ICA were enrolled. Of total 1470 coronary segments (147 segments of LMA, 441 segments of the LAD, 441 segments of the LCx, 441 segments of the RCA), 98.9% were eligible to be assessed and only 1.1% (15/1470) were ineligible due to very high calcium clumps and severe motion artifacts. Compared to the ICA, the overall sensitivity of the 256 MDCT in detecting coronary stenosis was 88.3 %, specificity was 96.1%, positive predic- tive value was 88.1 % and the negative predictive value was 96.2% with an overall accuracy of 94.2% (p=0.20). In massive calcium scoring cases (calcium scoring ≥400 U), the sensitivity of 256 MDCT in detecting coronary artery stenosis was 90.3%, specificity was 96.1%, positive predictive value was 87.5% and the negative predictive value was 95.5%; the overall accuracy was 92.9%. In nonmassive calcium scoring cases (calcium scoring
The 256 MDCT, regardless of calcium burden, offers a reliable diagnostic accuracy in assessing coronary artery stenosis.
256 MDCT angiography, Invasive coronary angiography (ICA), Calcium scoring, Coronary arterystenosis
10.31524/bkkmedj.2011.02.001