Electronic ISSN 2287-0237
It was for more than a century that the mysterious sudden death, so-called “Lai Tai”, had been prevalent among villagers in Northeastern (NE) Thailand. Most victims were otherwise healthy young men who died unexpectedly during sleep. Moaning and gurgling sounds had been heard before they became unre- sponsive and expired. In some families, similar deaths had been occurred to male siblings, for over four generations, which was suggestive of genetic preponderance. It was still a local myth that these unexplained deaths were caused by a widow ghost came to take the mens’ soul at night. Several years ago, Lai Tai received media attention after a cluster of deaths of Thai workers in Singapore. Despite extensive autopsies by local authorities, the cause of death remained unidentified. So far, Lai Tai had affected our nation in many ways, from the smallest unit where wives and children had lost their husbands, fathers and the heads of family, up to the national level, that lost the significant incomes from the death of workers.
In 1992, Lai Tai was brought to our attention by Professor Sumalee Nimmanit and colleagues who were studying the prevalence of kidney stones in people of the NE region. In 1994 we had an opportunity to examine the first victim of Lai Tai who had suffered sudden death from ventricular fibrillation. After that, serial investiga- tions under the direction of Professor K.Nademanee were conducted at Bhumibol Adulyadej Hospital and other centers such as Siriraj, Ramathibodi, Central Chest, Chulalongkorn and Khon Kaen. The findings are summarized below.
1. Arrhythmogenic marker, similar to Brugada’s syndrome (BrS)
Examination of a group of Lai Tai survivors in 1994 showed 90% of them to have typical ECG marker; abnormal repolarization in precordial lead (V1-3)1-3 resembling Brugada’s pattern (reported by Pedro & Joseph Brugada in 1992.4 This marker became normalized from time to time5 and could be enhanced by placing precordial ECG leads (V1-3) in higher position (in the 2nd and 3rd intercostal space)6 or by giving medication that blocks sodium ion channels.7, 8
2. Mechanism of sudden death is spontaneous ventricular fibrillation
In the pilot study, ICDs were implanted in 10 Lai Tai survivors and revealed the cause of death was spontaneous ventricular fibrillation (VF) that sometimes could be self-terminated1.9 Abnormal autonomic tone as displayed in our study might play a significant role in the night attack of VF in these patients.10
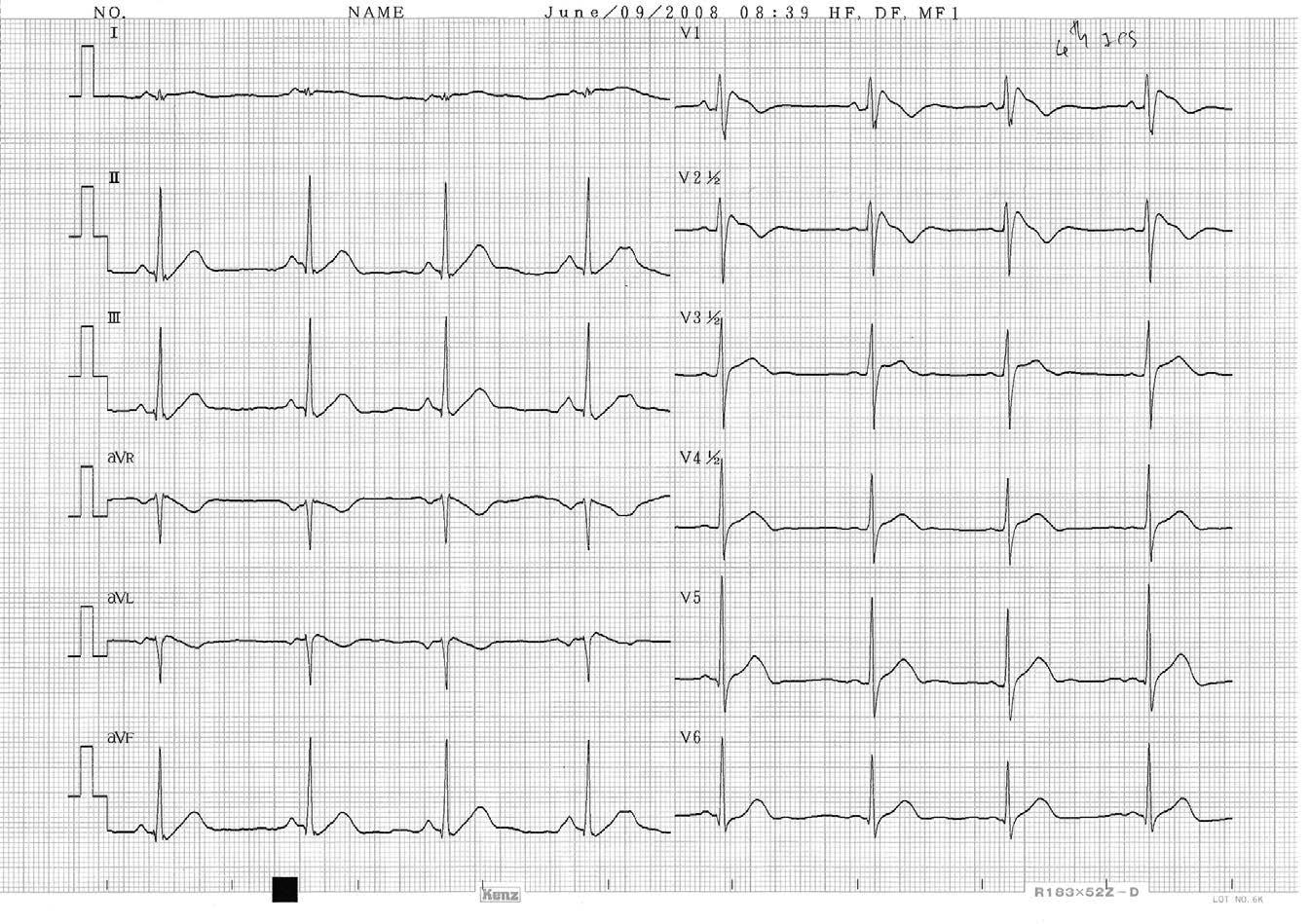
Figure 1: Typical ECG marker (coving type of ST segment elevation) in V1-2 found in SUDS or Brugada’s patients.
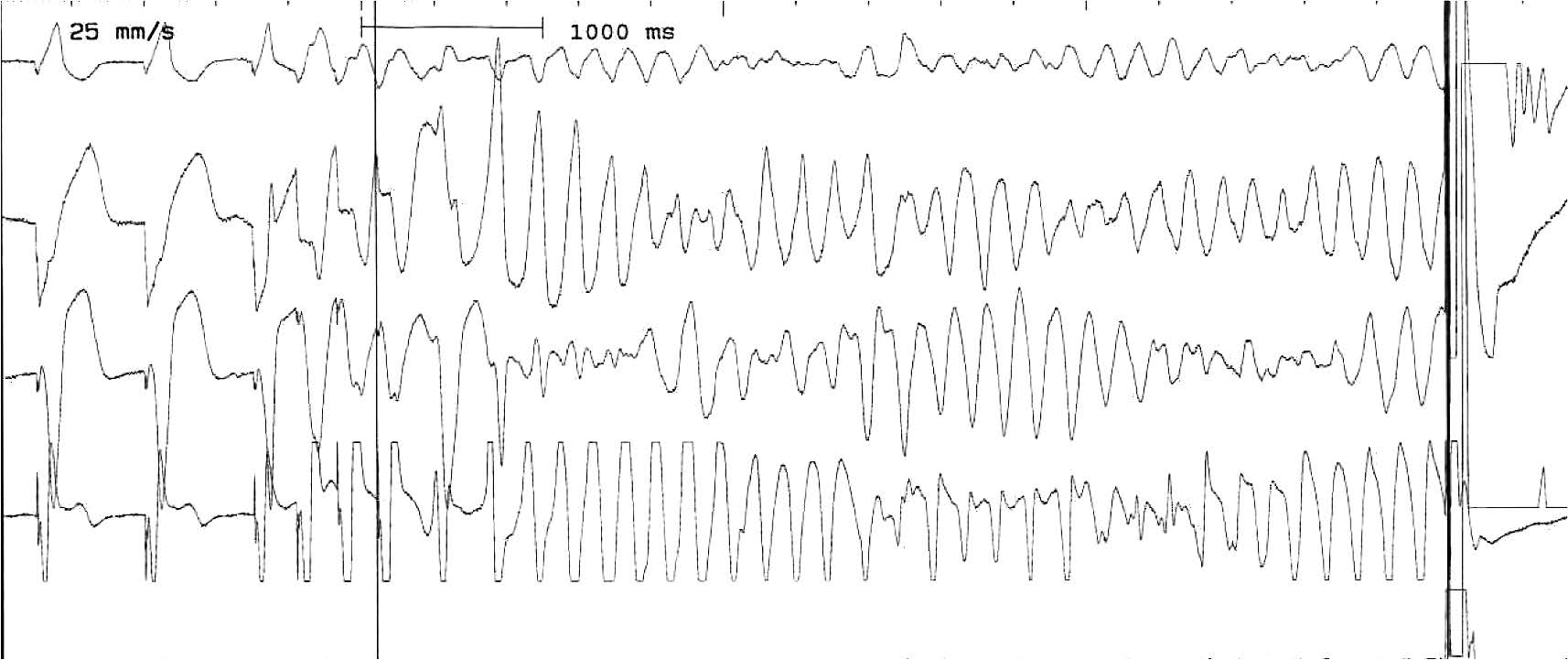
Figure 2: Inducible sustained VF in EP laboratory of one SUDS survivor required cardioversion.
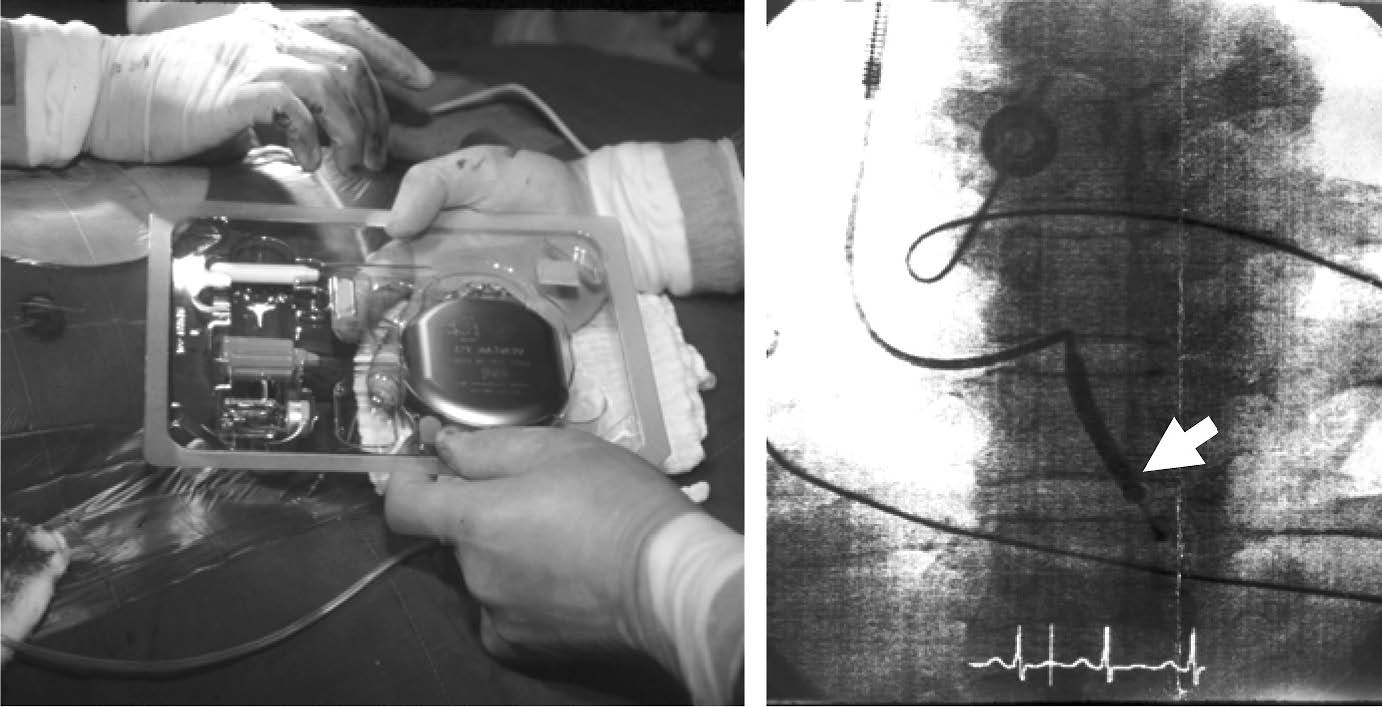
Figure 3: ICD device (A) and lead in right ventricle (B) see arrow.

Figure 4: Sustained VF was terminated by ICD shock in one Lai Tai survior
3, ICD saved lives and was more effective than β-blocker
The first randomized study (DEBUT) compared using implantable cardioverter-defibrilator (ICD) and β-blockers in Lai Tai survivors. The trial was however, prematurely terminated after an interim analysis by the Safety Monitoring Board, owing to the overwhelm- ing benefit of ICD over the drug (mortality in ICD 0% vs. β-blocker 14%, p=0.004).11 This trial was the first randomization comparison between device (ICD) and drug in normal structural heart victims and showed no mortality in ICD arm.
4. Genetic discovery of SCN5A mutation
The genetic collaboration work with J. Towbin and colleagues in Texas revealed the mutation of gene encoding sodium ion channel in one third of Lai tai and Pokkuri (sudden unexplained death in Japanese) family members.12 This mutation resulted in decreased or non-functioning of sodium ion channel that could explain the typical ECG changes in RV epicardium.13 Currently, there are at least nine genes found to be associated with this syndrome.
5. ICD may not helpful in asymptomatic BrS.
While it is clear that symptomatic BrS/SUDS patients need ICD treatment, controversy exists as to what to do with the asymptomatic cases with the Brugada ECG pattern. We have launched the SUDSPAC trial which is a randomized trial comparing prophylactic ICD implantation and no ICD treatment in asymptomatic BrS/SUDS patients. After five years follow up, we concluded that ICD offered no benefit since the mortal- ity of asymptomatic BS was quite low and did not reach statistical significance (ICD 0%, no ICD 2.3%, p=0.5).14
6. Arrhythmogenic substrate and epicardial ablation
Implantation of ICD is the only proven effective treatment for Lai Tai survivors, however, some patients still require anti-arrhythmic medication to reduce VF events. Despite medication, frequent ICD shocks from recurrent VF still occurred in some cases. Fortunately, in our recent study, with the advent of new mapping technology, we discovered that BrS/SUDS patients have VF substrate at the anterior aspect of the right ventricular outflow tract (RVOT), which manifests as low voltage-fragmented late potentials exclusively localized in the anterior RVOT epicardium. Radiofrequency (RF) ablations over this region not only eliminated the Brugada ECG pattern but also prevented VF episodes occurring, both spontaneously and during electro- physiologic studies. Our findings also shed light on the mechanisms of this disease; namely that the most important underlying electrophysiologic mechanism of the BrS/SUDS syndrome is delayed depolarization at the RVOT epicardium.15
How should we treat Lai Tai cases?
For the aborted sudden death cases and symptomatic patients, ICD is indicated. Reimbursement of the ICD is now available from all types of health insurance, in- cluding Social Welfare and National Health Security office. Patients should stop drinking alcohol, and check their potassium levels every 3-6 months as well as ICD interrogation. A high potassium diet is recommended if there are no other contra-indications. Cases of frequent VF should be admitted and treated with amiodarone, K, Mg should be kept within the normal range. In VF storm, quinidine or isoproterenol administration should be help- ful along with K and Mg supplements. Prompt contact with the DEBUT Center, Bhumibol Adulyadej Hospital or Pacific Rim Electrophysiology Research Institute at Bangkok Hospital is highly recommended for potential RF ablation.
In asymptomatic cases, current research did not support the prophylaxis ICD since the mortality is insignificantly low. Avoid alcohol beverages, regular potassium supplement are routinely recommended. In the present of having fever, antipyretic, supportive treatment, adequate K and Mg supplement are encouraged.
Currently, ongoing research is being conducted at DEBUT Research Center, Bhumibol Adulyadej Hospital and Pacific Rim Electrophysiology Research Institute at Bangkok Hospital under the support of Duang-Tawan Foundation and Vejdusit Foundation.









