Electronic ISSN 2287-0237
There are several methods for managing pancreatic cancer. Surgical resection gives the best chance for a possible cure in the early stages of the disease. However only 10-20% of patients present with potentially resectable pancreatic cancer. Chemotherapy is the treatment of choice for the advanced metastatic disease. For locally advanced, inoperable pancreatic cancer, combined chemotherapy and radiation is the preferred treatment.1 In the case of patients who have contraindications for surgery, concurrent chemoradiation may be chosen2. The patient in this study, was a case of adenocarcinoma at the pancreatic head, stage T1N0M0, with underlying heart disease; she thus was contraindicated for a major operation. The treatment plan was chemoradiation, using VMAT radiotherapy technique with a radiation dose of 45Gy in 25 fractions and oral Xeloda.
A 82-year-old female presented with obstructive jaundice. A CT scan of the upper abdomen revealed a 1.3 cm. soft tissue mass at distal common bile duct (CBD) and periampullary region causing compression and dilatation of common bile duct and pancreatic duct. The endoscopic ultrasound and fine needle aspiration together with Metallic stent placement was done. The pathologic findings showed malignant cells comparable with adenocarcinoma of the pancreas. The patient underwent further investigations which included a F18-FDG-PET/CT scan. (Figure 1) The scan demonstrated a hypermetabolic mass at the pancreatic head with a SUV of 4.9. Neither Distant metastasis nor regional nodal spread was detected. The patient was then treated with concurrent chemoradiation. Surgery was not a priority treatment, due to her heart condition.
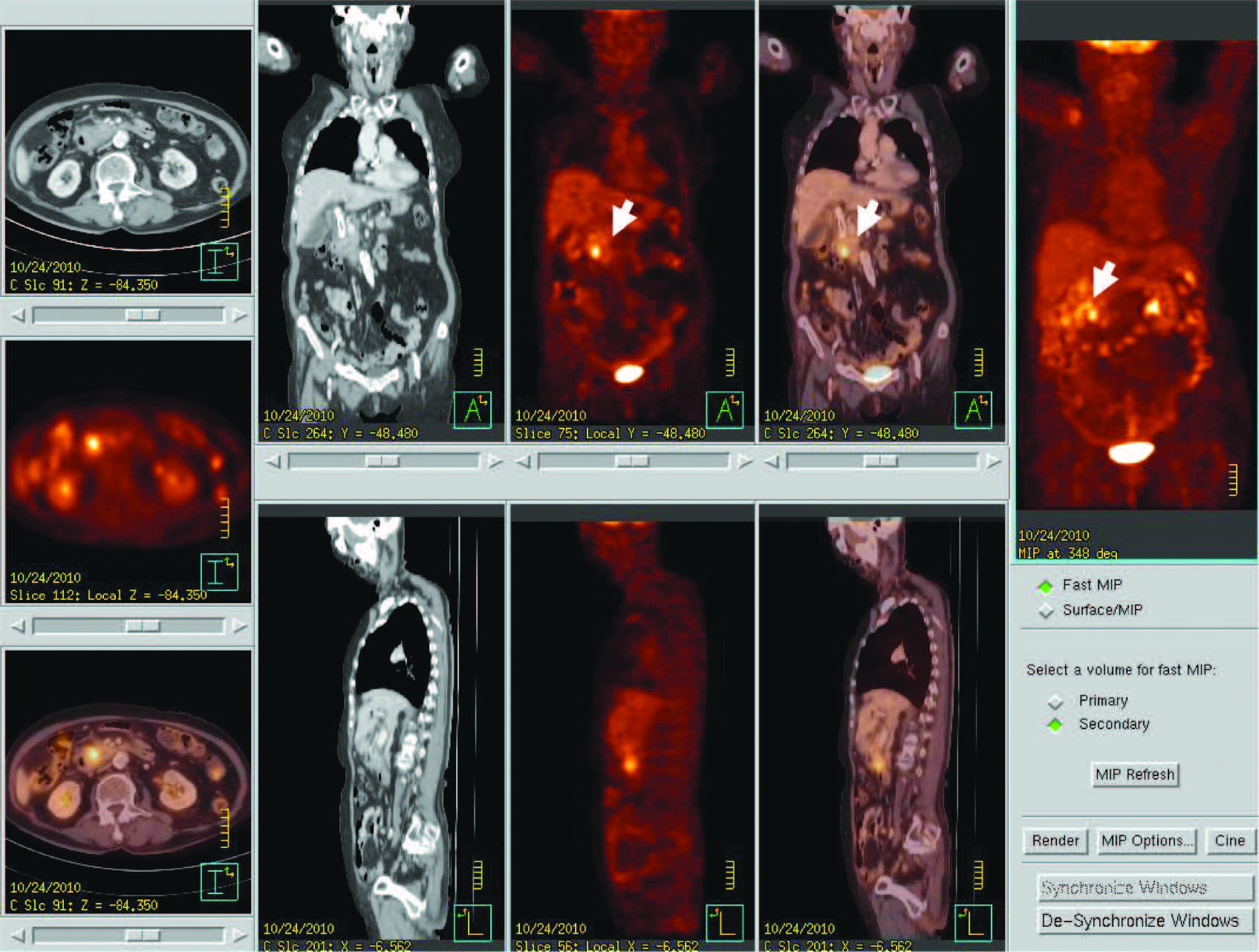
Figure 1: PET/CT images show 1.3 cm. hypermetabolic mass at pancreatic head (arrow), without regional node and distant metastasis (stage T1N0M0)
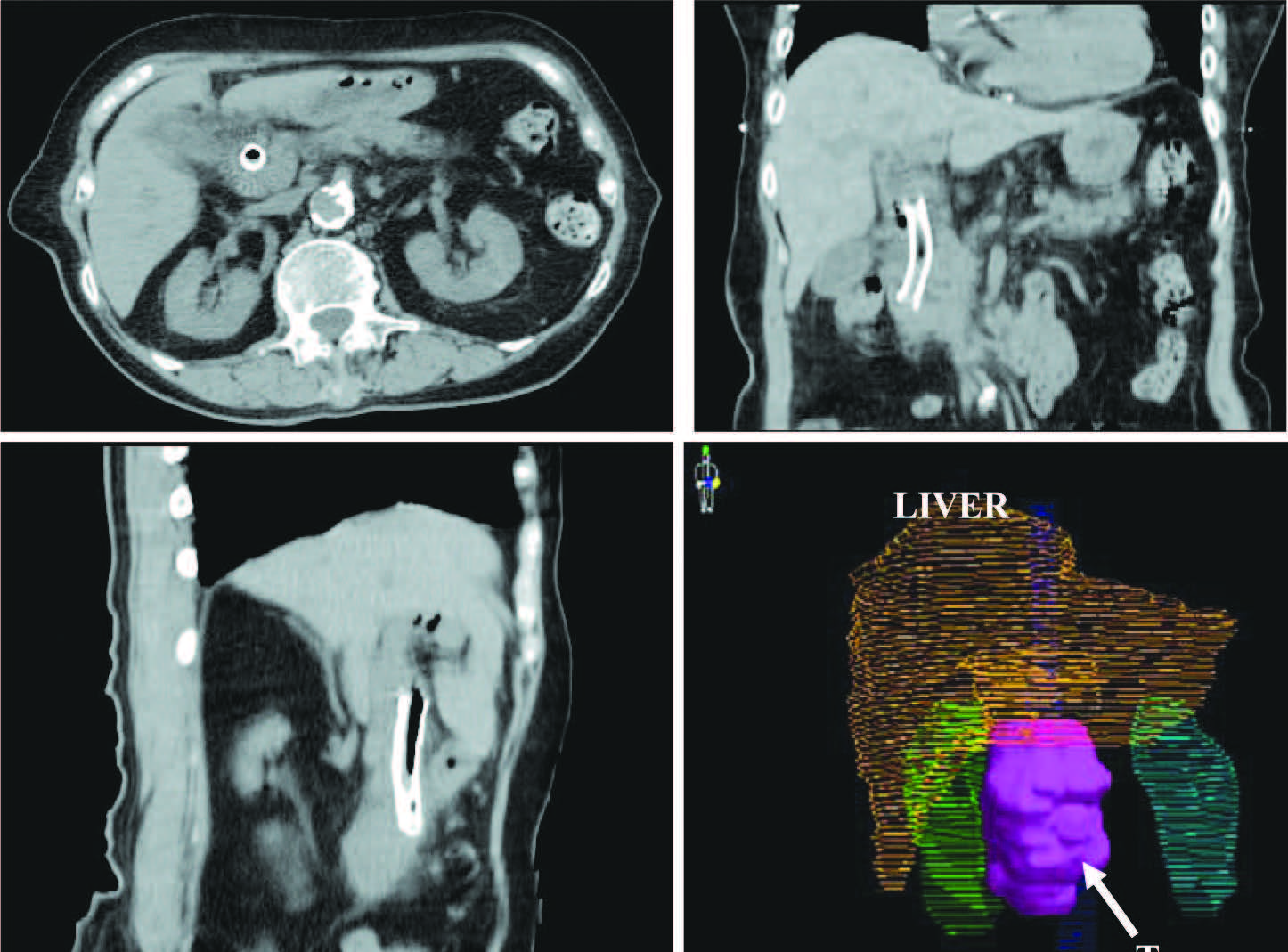
Figure 2: CT images show the tumor in 3 plane and 3 Dimensional imaging of tumor (pink colour), OAR Liver (yellow), right kidney (green), left kidneys (blue). There is metabolic stent placement in common bile duct.
A single arc VMAT, planned by CMS Monaco® treatment planning system, version 2.03 (Elekta Group St. Louis, MO), was used for radiation treatment. We compared the results of the VMAT plan with conventional IMRT plan (5FIMRT) planned with the same TPS (CMS Monaco®). The total number of monitor units (MU) per fraction decreased from 543 to 494 MU and significantly reduced treatment time from 15-20 minutes to 5 minutes, due to a higher dose rate and continuous beam on during modulated arc radiation.
The total prescribed dose of radiation for this case was 45 Gy with a total of 25 fractions. The PTV volumes covered by at least 95% of the prescribed dose were 98.91% and 99.62% respectively, for the VMAT and IMRT plan. In terms of critical organ sparing, V20 (the volume received 20 Gy dose) for the liver in VMAT plan was reduced from 13.20% to 7.75%, V20 for the right kidney was reduced from 3.24% to 1.49% and V20 for the left kidney and the spinal cord dose was comparable to IMRT plan (Table 1). The 2D dose distributions for transverse, sagittal, and coronal planes are shown in Figure 3.
Table 1: Comparison of IMRT and VMAT plan
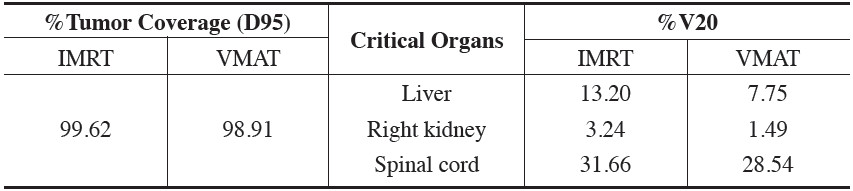
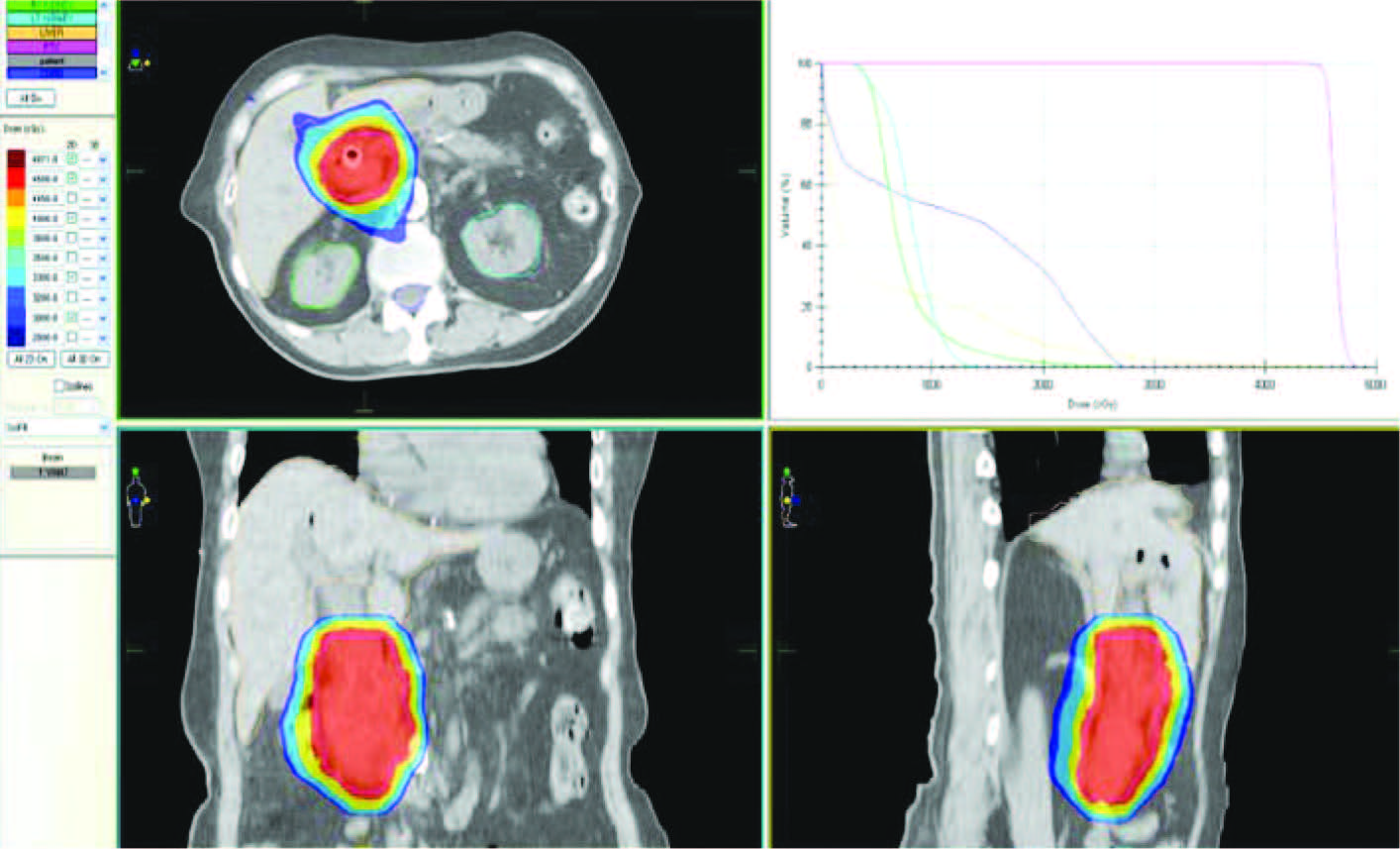
Figure 3: The 2D distributions for transverse, sagittal, coronal planes and Dose Volume Histograms (DVHs) of VMAT plan
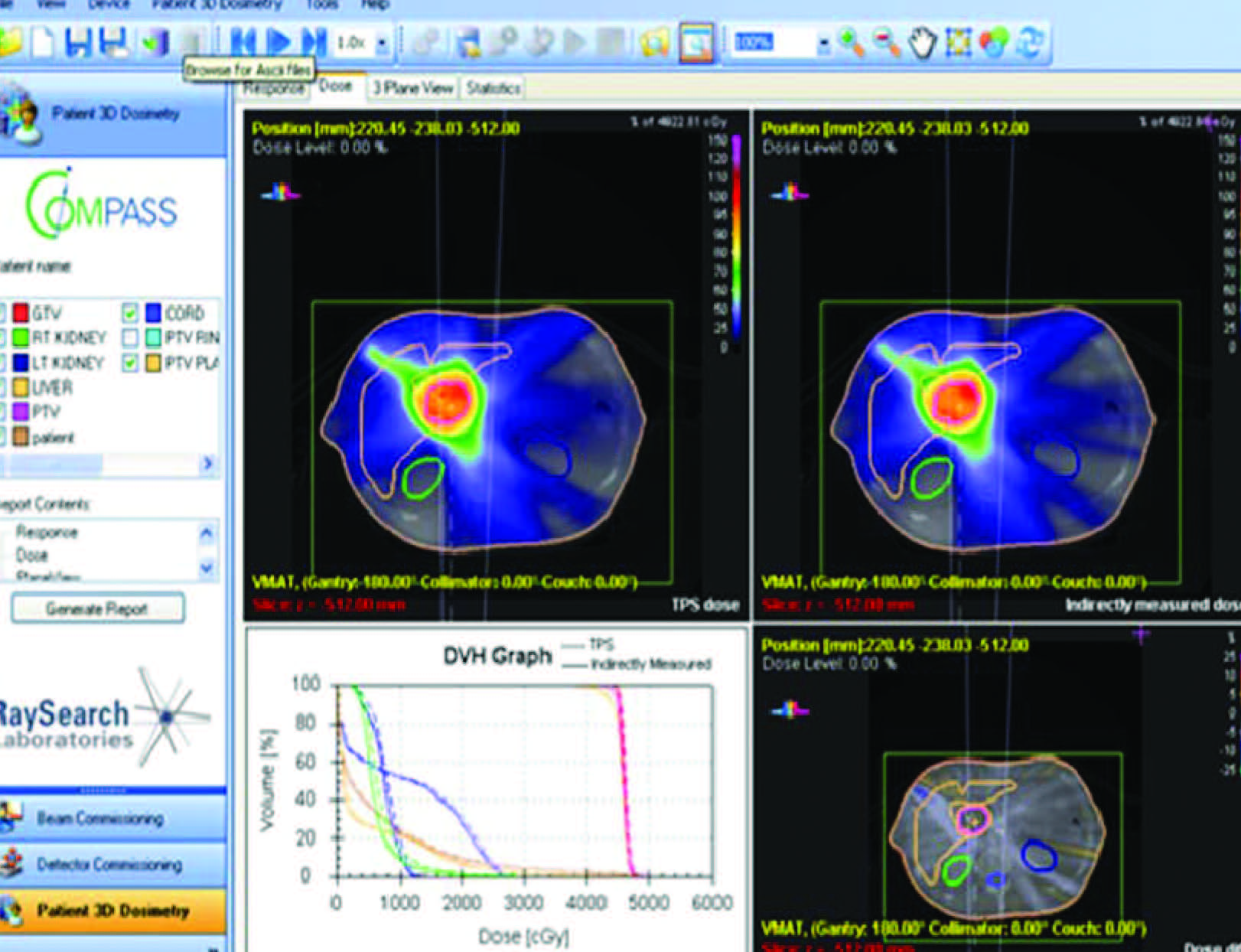
Figure 4: Shows the result of COMPASS 3D QA for VMAT plan
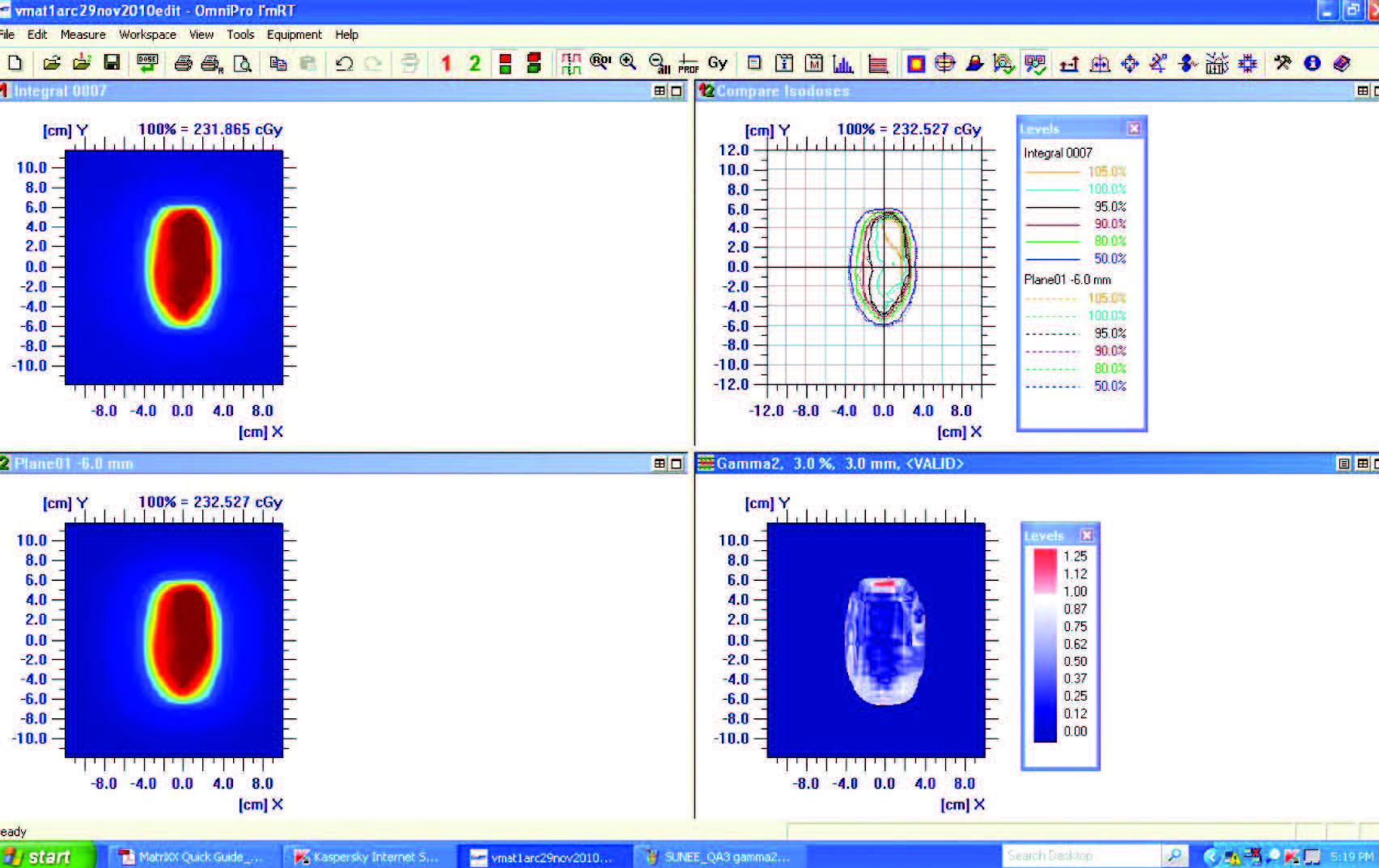
Figure 5: Shows the result of 2D QA for VMAT plan with Omnipro IMRT
VMAT plan QA was performed in both 2D and 3D QA analysis, using MatriXX Evolution ionization chamber array and Compass 3D verification software (IBA Dosimetry, Schwarzenbruck, Germany). 3D and 2D planar dose QA were analyzed with Omnipro IMRT software. The 3D dose distribution reconstructed in the patient’s anatomy (Figure 4), showed that the difference between TPS calculation and the measurement in terms of the average dose and average gamma in PTV was 0.43% and 0.37 respectively. The 2D dose distribution for coronal plane was measured and compared, the agreement between the measured and calculated dose distribution was within 98% using gamma criteria 3%/3mm. (Figure 5) The point dose was measured with 0.125 cc. ion chamber (PTW Freiburg, Germany), the difference was less than 3% (-2.79% in this study). These results indicated the VMAT plan could be delivered accurately using Elekta Synergy VMAT linear accelerator.
The verification of patient and target position used Elekta IGRT technique, XVI® cone beam CT. The patient underwent XVI® image guidance daily for the first three days of treatment and then once a week. The result for mean systemic/random setup error in translation direction for this patient was -0.1±0.07 SD, 0.36±0.19 SD and -0.24±0.16 SD in x/(R-L), y/(S-I) and z/(A-P) respectively. The position correction is neglected if less than 0.5 cm error in any direction. The total irradiation time for VMAT 1 arc is 5 minutes for 494 MU.
Outcome and follow-up
After the completion of the treatment, the patient was free of disease during the 6 months follow up period. The liver function test appeared normal, bilirubin declined to normal levels: C19-9 decreased from 626.50 units/ml. to 178.40 units/ml.
The treatment of pancreatic cancer depends on stage, patient status and co-morbidity, but usually requires multi- modality of treatment. One combined treatment method is concurrent chemoradiation therapy; the treatment has been demonstrated not only to palliate symptoms but also to improve patient survival. Nowadays, radiation therapy plays an important role in cancer treatment, using high energy x-rays or other types of radiation to kill cancer cells or keep them growing. The challenge of radiation treatment is the acute radiation side effects on surrounding critical organs, such as kidney, liver or the spinal cord.
Radiation therapy began to be used for cancer treatment more than 100 years ago3. The radioactive source, Radium was employed and later, Cesium and Cobalt 60 were also used. Between 1948 and 1953 the first linear accelerators (Linac) were used as sources of radiation.
Atotal radiation dose is typically divided into multiple sessions (fractionation). As such, there is a need to repeatedly place the radiation beam accurately and reproducibly on the target volume. This has been achieved through a variety of image guidance techniques. Treatment planning is the process used to define the incident angles, shapes and intensities of the Radiation beams used to irradiate the tumor. The development of two-dimensional computed tomography (CT) enabled radiation oncologists and neurosurgeons to directly visualize tumors. Without these early treatment planning systems, the ability to define the tumor using only two-dimensional images was limited and it was impossible to visualize.
Computerization has led to immense leaps in radiation therapy and is now an invaluable tool, in parallel with the great developments in imaging technology and radiation technologies.
The fast development of advanced imaging and radiation therapy have enabled new state of the art treat- ment techniques, namely IMRT (intensity modulated radiation therapy) IGRT (image guided radiation therapy) and then VMAT (volumetric modulated arc therapy) (Figure7)

Figure 7: The Elekta Synergy® combines VMAT&IMRT and image guided radiation therapy (IGRT), XVI®
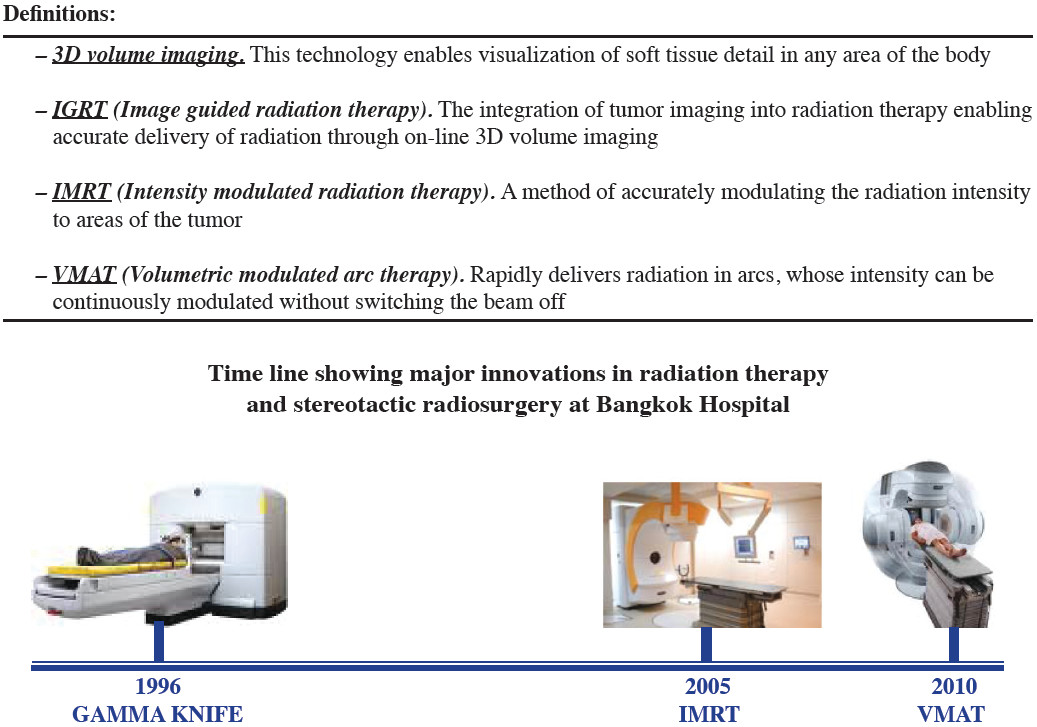
Three dimensional conformal and IMRT (Intensity Modulated Radiation Therapy) treatment is currently used to reduce acute short term side effects. IMRT represents one of the technical innovation in modern radiation therapy which uses non-uniform intensity patterns with computer aided optimization to achieve superior dose distribution.
Recently, the sophisticated and advanced radiation therapy technique called Elekta VMAT (Volumetric Modulated Arc Therapy, which was installed in Bangkok Hospital in March 2010) has become an alternative choice for pancreatic cancer treatment in unresectable cases or where surgery is contraindicated. VMAT allows a similar or more precise dose distribution and faster dose delivery than IMRT.
VMAT produces irradiation with simultaneously varying dose rates, gantry speed, collimator, and leaf positions. It’s integration with IGRT technology (XVI®, X-ray Volume Imaging), provides three dimensional volume imaging to increase precision, accuracy of target position and therefore clinical confidence. This case study of treating pancreatic cancer with Elekta VMAT planning, shows the dose distribution to the tumor is comparable to IMRT technique but with better organ preservation,whilst also significantly shortening treatment time.
In our case study, the patient with cancer at the head of the pancreas stage T1N0M0 was treated with VMAT for curative dose and normal organs such as liver, spinal cord and kidney tolerated the procedure very well. VMAT is thus an important development in treatment options when radical surgery is contraindicated.









