Electronic ISSN 2287-0237
An acute isolated lateral leg compartment syndrome with peroneus longus muscle tear associated with deep peroneal nerve palsy has been reported to occur after a sport and non-sport injury. The patient might present at the emergency room or orthopedic department complaining of pain, tingling or burning sensation or paresthesia in the skin, tightness in the muscle, numbness or paralysis of part of the limb. However, a high degree of suspicion is necessary to establish the diagnosis early on in its course to avoid potentially disabling sequelae. A precise physical examination regardless of the investigation used, together with compartment pressure measurement, is most useful in cases where the clinical examination is uncertain.
A 25-year-old male badminton player from a badminton club presented at the emergency department (ER) complaining of left lateral leg pain for four days. He suffered an inversion injury to his left ankle during a badminton game and gradually developed pain which was not under control with medication. Four days post injury he sought medication from the ER due to the increasing pain on the lateral of his left leg. His pain was out of proportion given the amount of swelling of his leg. On physical examination, his leg was moderately tender over the lateral part; the pedal pulse and posterior tibial pulse were present. The range of motion was decreased to zero from five grade of power of tibialis anterior (TA), extensor hallucis longus (EHL) and extensor digitorum longus (EDL) muscle and the pinprick sensation test at the areas of deep and superficial peroneal nerve distribution were decreased, and the inversion stress test (IST) was also negative. An ultrasonography was also performed at the bedside due to the moderate swelling of the muscle, and then the hematoma was detected (Figure 1-2).
The compartment pressure measured by White-Side Infusion Technique1 was eighty mmHg, so a compartment syndrome of lateral leg was immediately diagnosed, and then the patient was taken for urgent lateral fasciotomy (Figure 3). The peroneus longus muscle still showed minimal capillary perfusion and tested positive to the muscle contraction test. The presence of tissue viability is the reason to keep the muscle by anastomosed of the sheath to the peroneus brevis and the primary closure was delayed by shoelace suture technique. Three days after the operation, signs of tissue necrosis were detected so the peroneus longus muscle was completely removed and a secondary closure (Figure 4) was done, and totally stitched off over the next ten days.
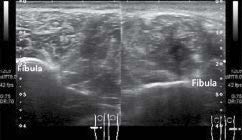
Figure 1: The cross sectional view of lateral leg ultrasonography (left), normal lateral compartment in the right leg (right). The left lateral leg presented with a hematoma.

Figure 2: The lateral view of left lateral leg ultrasonography, where a large hematoma was detected.

Figure 3: Intra-operative photograph of left lateral leg, showing the complete torn peroneus longus musculotendinous junction

Figure 4: Intraoperative Finding of the second operation, the Peroneus longus muscle was totally removed and other com- partments were normal, the superficial peroneal nerve was also identified

Figure 5: The active movement of the left foot, with regards to the recovery of motor power of tibialis anterior (TA) and extensor hallucis longus (EHL) and extensor digitorum longus (EDL) muscle at fourteen weeks, and at thirty two weeks when the physical therapy course ended.
For full motor function, throughout the day and night, ankle foot orthosis (AFO) was required since at day thirty-five post operation foot drop presented as a result of palsy of the deep peroneal nerve. The motor function was developed from grade zero of TA, EHL and EDL to grade five, one and five at fourteen weeks later (Figure.5), and EHL power improved to grade four at thirty two weeks respectively. However, as his ankle was able to present in the natural position, he can walk and run well but is still unable to return to the badminton courts.
The acute isolated lateral leg compartment syndrome with the peroneus longue muscle tear and deep peroneal nerve palsy is rare2 and especially in the sport injury in even high or low energy of the mechanism.2-5 Muscle swelling and pain are the chief complaints that bring the patient to the hospital or if they do not find relief from analgesic remedies. Some cases often occur as chronic compartment syndrome or they have more tolerance to the pain compared with other patients, at this point the emer- gency physician should be more concerned. The gradual development only at the part of lateral leg compartment syndrome is very difficult to discern and usually leads to delayed diagnosis. In the many case reports, the patient seeks medical support6 very late and in some cases presented to the hospital with the compartment syndrome associated with peroneal nerve palsy.6-8 The key point of this case report is the loss of inversion stress test, and being alert for any complaint of pain that is out of proportion with the leg swelling, as even though ultrasound was done, this is ordinarily not used for diagnosis, but in emergency situations, ultrasound is one non-invasive study available. The compartment pressure increased following the injury and the study of direct measurement techniques shows the normal pressure of a tissue compartment falling between 0 to 8 mmHg. Diminished capillary blood flow occurs when the tissue pressures reach between 20-30 mmHg. Many orthopedic physicians used the ACS delta pressure (diastolic blood pressure minus measured compartment pressure) at 30 mmHg to determine the need for fasciotomy but many believe the use of absolute measurements leads to unnecessary fasciotomies. The continuous invasive monitoring of alert patients may alow physicians to observe their symptoms and to closely follow up. This may avoid the performance of an unnecessary fasciotomy. The onsite non-invasive measurement such as ultrasonography to detect the size of hematoma and the increase in compartment pressure that lead to the compartment syndrome is questionable in this case. However, further study is advised.
A case presentation of a rare occurrence of acute lateral leg compartment syndrome associated with a tear of the peroneus longus muscle and deep peroneal nerve injury due to inversion of ankle in a sport injury. Increasing pain at the lateral aspect of the leg and loss of inversion stress test are observed. The increase of lateral leg compartment pressure strongly indicated acute compartment syndrome. Then an immediate fasciotomy was performed followed by a full course of physiotherapy, and the patient recovered over time.









