Electronic ISSN 2287-0237
Food allergy is defined as “an adverse reaction to food in whichimmunological mechanisms have been demonstrated.” 1 Theincreae in the prevalence of food allergy was reported as about3.5%-5% of the general population 2 and 8% of the paediatricpopulation.3 The characteristic of food-induced allergic disordershave been defined as IgE-mediated, cell-mediated and mixed(IgE and cell-mediated).2 Prevalence of adverse reactions to fruitswas reported in 2.2-11.5% of children and 0.4-6.6% of adults.4 Amongfresh fruit, banana is not a common cause of fruit allergy, but it cancause life-threatening symptoms. Banana allergy is characterized asbanana hypersensitivity, cross reaction to birch tree or pollen knownas oral allergy syndrome and the latex-fruit syndrome which oftenoccurs in patients sensitive to latex. Here we reported a case of apatient who experienced banana anaphylaxis without latex or pollenallergy and can tolerate baked banana.
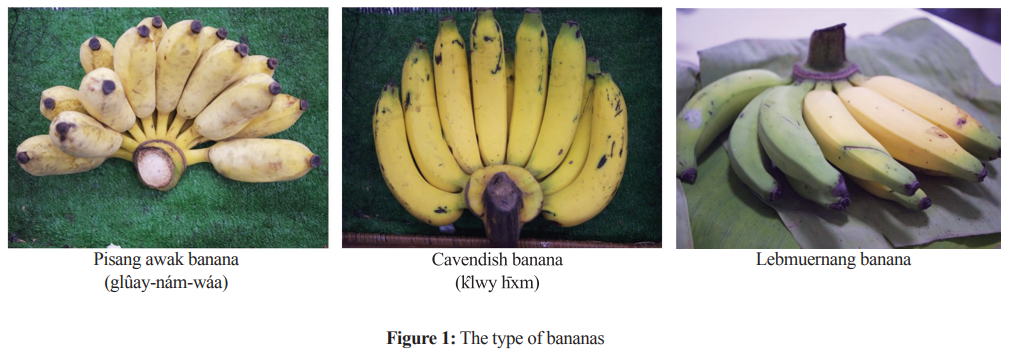
A case of 59-year-old Thai woman with generalized pruriticurticarial rash, rhinorrhea, nasal obstruction and shortness of breathafter 30 minutes following the ingestion of two pieces of raw Pisangawak banana (glûay-nám-wáa) (Figure 1) together with paracetamol1,000 mg. At the emergency room, blood pressure 160/90 mmHg,pulse rate 80/min, respiratory rate 15/min, body temperature 37.2°C.The physical examination revealed good consciousness, endexpiratory rhonchi both lungs, nasal swelling, angioedema botheyelids with generalized urticarial rash, and organ presented withinnormal limits. Food-induced anaphylaxis was diagnosed andadrenaline (1:1,000) 0.5 mL intramuscular was given to herimmediately with the rapid response of her clinical syptoms withinan hour. Unfortunately, a late phase reaction occurred 3 hours later.She was then admitted as an inpatient for a day and discharged withself-epinephrine auto injection. Serum tryptase 2 hours after theonset of reaction revealed 19.10 ug/L (1.9-13.5).
She was referred to the allergy clinic at Ramathibodi hospital for further evaluation to ascertain the cause of anaphylaxis. A complete history was taken and this found that she had experienced two anaphylaxis events in her
life. The first event was five months prior to this reaction, happened after she ate raw Pisang awak banana and
mushroom for 1 hour, she had the same response (nasal swelling, angioedema both eyelids with urticarial rash) and was treated with intramuscular adrenaline (1:1,000) 0.5 mL. After this event, she avoided mushroom and banana. The second anaphylaxis event as described above. After this event, the patient was self-administering paracetamol without any reaction and still avoiding all bananas.
She suspected banana anaphylaxis from her history and laboratory investigation. She can eat all kinds of fruits such as jackfruit, kiwi or chestnut without any reaction. She can apply latex gloves or latex balloon as usual. We also evaluated others allergic diseases which found that she had non-allergic rhinitis and her underlying disease was seizures; her current medications were phenytoin, clonazepam and aspirin.
At the preliminary investigation for banana anaphylaxis,we performed the skin prick test. The histamine and normal saline were used as positive and negative control respectively. Skin prick test was considered positive when a wheal of more than 2 mm in diameter presented after 15 minutes. The result of skin prick test using commercial food allergens (ALK®) showed positive (4 mm) which was relevant to her symptoms and negative for mushroom. Other allergens including black pepper (3mm), peanut (3 mm), soybean (5 mm) and garlic (4 mm) were positive results but she is able to eat these foods without any allergic reaction.
To improve the accuracy of the skin test, we performed prick to prick skin test using raw Pisang awak banana, which revealed strongly positive 21 mm wheal size with a pseudopod. The specific IgE immunoblot for food profile and specific IgE to peanut were all negative. Eventually, the specific IgE to latex (ImmunoCAP®) was class 1 positive without clinical relevancy, so we performed the latex application test which presented a negative result. The latex allergy was excluded. We did not perform oral raw Pisang awak banana challenge test due to convincing history and laboratory result of anaphylaxis. We diagnosed banana anaphylaxis and advised to avoid all kinds of banana.
Later, she accidentally ate an amount of baked Cavendish banana cake (Khêk klwy hxm) without any reaction. This was surprising given her history. So the prick to prick skin test with raw Cavendish banana and Lebmuernang banana (Figure 1) were performed which showed strongly positive results (18 mm, 10 mm of the wheal size with pseudopod, respectively). But a negative result was found to baked banana (Cavendish banana in a banana cake and Pisang awak banana in a Thai bakery baked banana with sticky rice or Khaotummud). We performed the oral food challenge test to confirm the tolerability to baked banana and the result showed she could eat one and a quarter cups of the baked Cavendish banana and two pieces of Khaotummud (baked banana with sticky rice) without any reaction.
In summary, the final diagnosis was raw banana anaphylaxis, we advised a patient to avoid all kinds of raw bananas but could eat all sorts of baked banana and should always carry a self-epinephrine autoinjection kit.
Banana allergy has a diverse spectrum of reactions from mild to life-threatening symptoms depending on the sensitized allergens. Some cases of banana anaphylaxis can tolerate baked banana









