Electronic ISSN 2287-0237
In cases of liver mass such as hepatoma or cholangiocarcinoma which are common in South-East Asian countries, many cases develop abdominal symptoms at the stage which is late for surgical intervention.1, 2 Today, using the technology of computed tomography (CT) study, and 3D reconstruction of liver volume using 3D software enables us to study the boundary of tumor mass as well as visualize the major vessels. The total volume of the liver and the total volume of tumor mass can thus be calculated pre-operatively. This kind of investigation enables better surgical planning and may be a good predictor of the possibility of post operative liver failure.3
A 74-year-old man presented with epigastric oppression, no nausea or vomiting. He had a physical check up, during which a liver lesion was found. The findings of the pertinent laboratory investigations, which included liver function tests were within normal limits. The immunology study revealed alpha-fetoprotein (AFP) 2.97 IU/mL. (0-7.22), CEA 2.70 ng/mL. (0-3.0). The CT of abdominal area showed an ill-defined hypodense mass with neovasculature stain at hepatic segment 3, measuring 4.5 x 3.5 x 2.9 cm. in greatest axial and coronal dimensions. The portal, right and middle hepatic veins as well as inferior vena cava (IVC) are patent. (Figure 1)
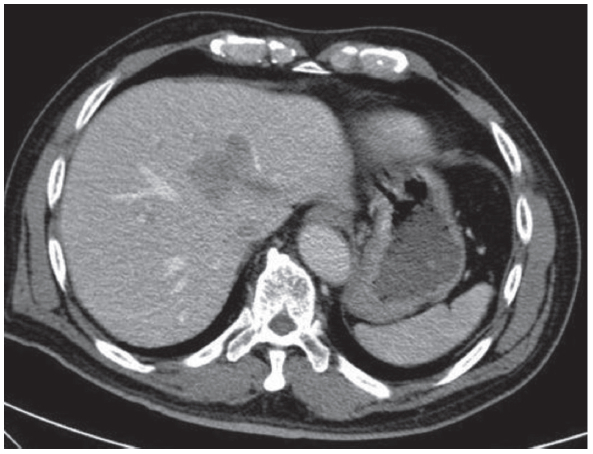
Figure 1: The CT of abdomen showed an ill-defined hypodense mass with neovasculature stain at liver segment 3, measuring 4.5 x 3.5 x 2.9 cm.
The 3D reconstruction of liver (Figure 2A-C) demonstrated the size of liver mass at left lobe in correlation to hepatic vein and portal vein; the total volume of liver was 1,411.50 cc., liver mass left lobe was 90 cc. Positron Emission Tomography and Computed Tomography (PET/CT) scan (Figure 3A-C) showed liver mass at segment 3 of liver with increasing metabolic activity SUV of 5.1. No 18F-fluorodeoxy-glucose (18FDG) avid lymph-node in the abdomen was seen. No 18FDG avidity in each lung, mediastinum or hilum was observed.
The patient underwent an exploratory laparotomy and left hepatic lobectomy.
The hepatic tumor was located near the inferior vena cava, no evidence of lymph node enlargement was observed. He had an uneventful post operative course. The gross specimen of mass at left liver lobe (Figure 4A) showed a tumor which was margin free from IVC 0.1 cm. IVC was intact, right and middle hepatic and portal veins were intact. The microscopic examination (Figure4B-C) revealed adenocarcinoma, well differentiated, compatible with infrahepatic cholangiocarcinoma, intraductal papillary neoplasm with associated invasive carcinocoma, mass forming type, nuclear grade II, tumor size 3.5 cm in greatest dimension. The follow up after surgery (see Figure 5 and 6A-C) showed complete removal of the tumor. The surgical margin was clear. IVC was intact. The 3D reconstruction of the liver showed all right lobe appearance normal, middle and right hepatic and portal veins are intact.
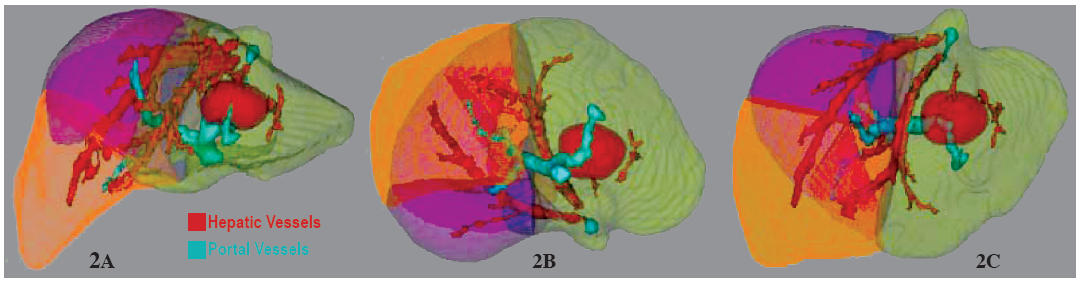
Figure 2A-C: The 3D reconstruction of liver with demonstrated the size of liver mass at left lobe in correlation to hepatic vein (red) and portal vein (green)
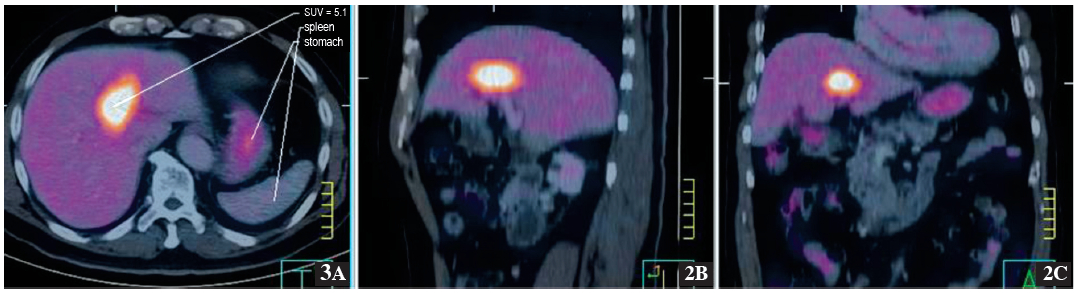
Figure 3A-C: The PET/CT scan showed liver mass at segment 3 of liver with increasing metabolic activity SUV of 5.1.
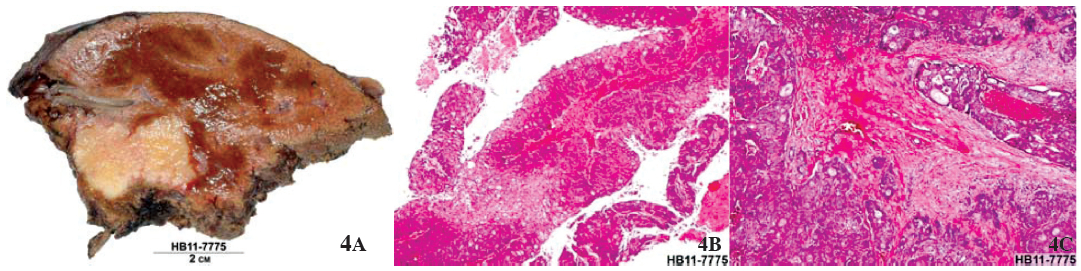
Figure 4A-C: The specimen (4A) showed a liver mass. The microscopic examination (4D-C) revealed adenocarcinoma.
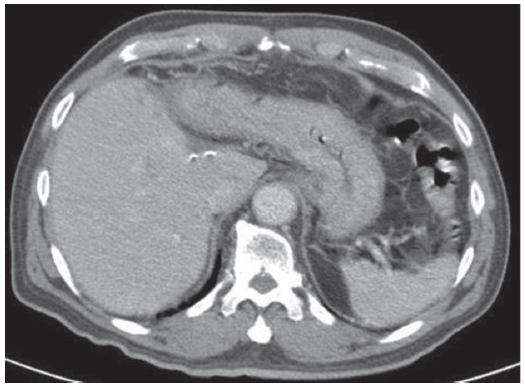
Figure 5: The CT of abdomen with contrast enhancement revealed status post left hepatectomy, No evidence of tumor recurrence at surgical margin is observed. IVC is intact.
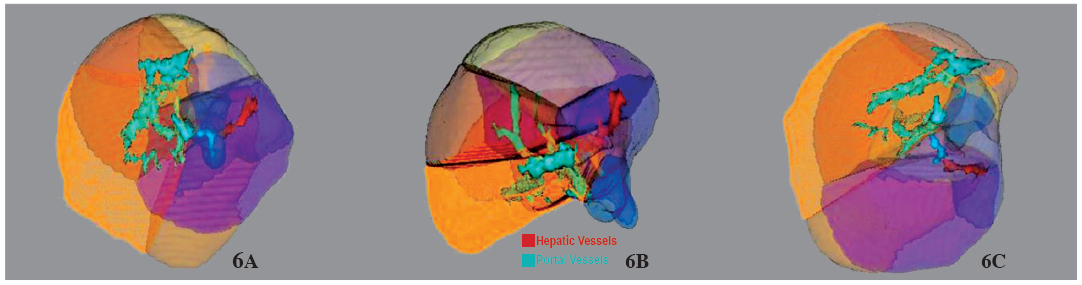
Figure 6A-C: The 3D reconstruction of liver post left hepatectomy, patency of hepatic vein (red) and portal vein (green) are seen.
The 3D reconstruction of the liver has to evaluate the total volume of liver, volume of tumor mass and vascular distribution including hepatic and portal veins. These considerations are very helpful for surgeons preoperative planning. In this case the tumor invaded only the left hepatic vein. Other veins were well preserved. This indicated a good prognosis. Hence, only a left hepatectomy which sacrificed the left hepatic vein was performed.
The 3D reconstruction of liver mass for liver analysis to evaluate the liver segmentation, vessels, territories and lesion provides very helpful information to enable better surgical planning and is a predictor of prognosis.









