Electronic ISSN 2287-0237
Futsal is a variant of soccer played indoors and was approved by FIFA (Fédération Internationale de Football Association) in 1962.1 It has become increasingly popular worldwide and there are less severe injuries to players that at soccer tournaments. There are fewer tackles in futsal than in soccer. Players who are in their early teens are most susceptible to injury, especially damage to knees, legs and ankles. Futsal players can often be injured because they have not warmed up sufficiently before starting to play, or because of sudden acceleration and deceleration moves that cause muscle tears. Plantar fasciitis is a painful swelling caused by a minor tear of the plantar fasci (a connective tissue on the sole of a foot) and is the most common injury in futsal players.2,3
In July 2012, the Bangkok Hospital opened the Bangkok Academy of Sports Exercise Medicine (BASEM). This new center contains a wide array of advanced diagnostic technologies and exercise equipment designed to optimize athletic performance and to aid faster rehabilitation. The unit also helps athletes to improve their fitness levels. BASEM is an accredited FIFA medical center of excellence and provides the same high standard of care at multiple centres worldwide in Europe, the United States, Australia, South Africa, Japan and Qatar.
BASEM is well equipped with top of the line sports exercise medical equipment. When injuries happen, BASEM can offer medical services and advanced treatment for many sports injuries. Treatments include tennis elbow release, knee arthroscopy for anterior cruciate ligament (ACL), posterior cruciate ligament (PCL) and meniscectomy, knee arthroscopy debridement for osteoarthritis (OA), shoulder arthroscopic decompressions and shoulder arthroscopic rotator repair. Specialists, including post-operative physiotherapists, are available around the clock.
The last futsal world tournament took place in Thailand from November 1-18, 2012. At the tournament, three futsal players sustained serious injuries and were treated by the team at BASEM.
A 35-year-old man presented with a painful left leg after taking part in the futsal 2012 competition. The magnetic resonance imaging (MRI) of the left leg revealed a grade 2 partial muscle tear of a deep section of the soleus muscle (Figure 1A, B) and a tear at the superficial section of the flexor hallucis longus muscle.
A thin layer of fluid (2.5mm wide, Figure 1C) could be seen along the interfascial plane.
At the fascia there was no tendon involvement, and there was increased signal intensity in the anterior surface of solens muscle. The patient responded well to symptomatic and conservative management.
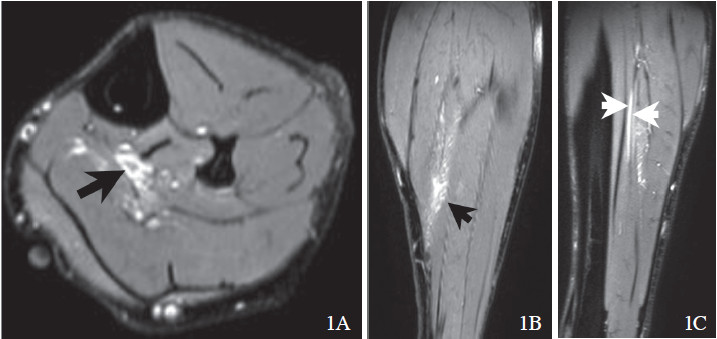
Figure 1 A,B: A thin layer of fl uid can be seen along the interfascial plane (black arrow).
Figure 1C: A thin layer of fl uid can be seen along the interfascial plane (white arrow).
A 31-year-old futsal player sustained a blunt injury to the left leg. He developed a painful swelling in his left calf for two days. The MRI of the left leg revealed a grade 1 partial tear of the muscle (Figure 2A) and of the musculotendineous junction of the medial gastrocnemius muscle. A thin layer of fluid (4mm wide, Figure 2B) was seen along the superficial fascia.
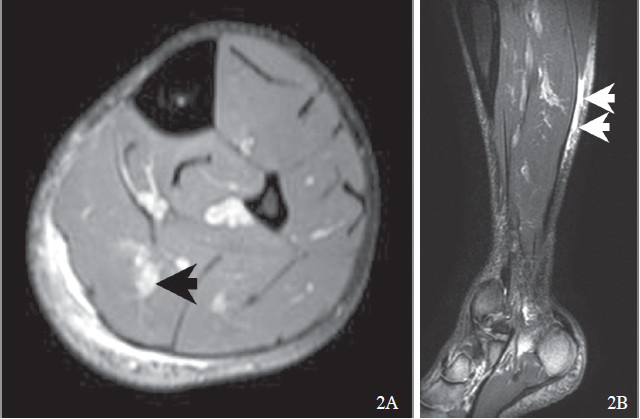
Figure 2A: MRI imaging shows a grade 1 partial muscle tear of the musculotendineous junction of the medial gastrocnemius muscle (black arrow).
Figure 2B: A thin layer of fl uid can be seen along the interfascial plane (white arrow).
A31-year-old futsal player sustained a blunt injury above the left thigh.He developed localized pain and tenderness The MRI of the pelvis showed a grade 1 partial tear of the left adductor longus muscle and tendon (Figure 3) at the superior pubic ramus insertion with fluid (1.5cm wide) along the superficial fascia of the muscle. He responded well to conservative management.
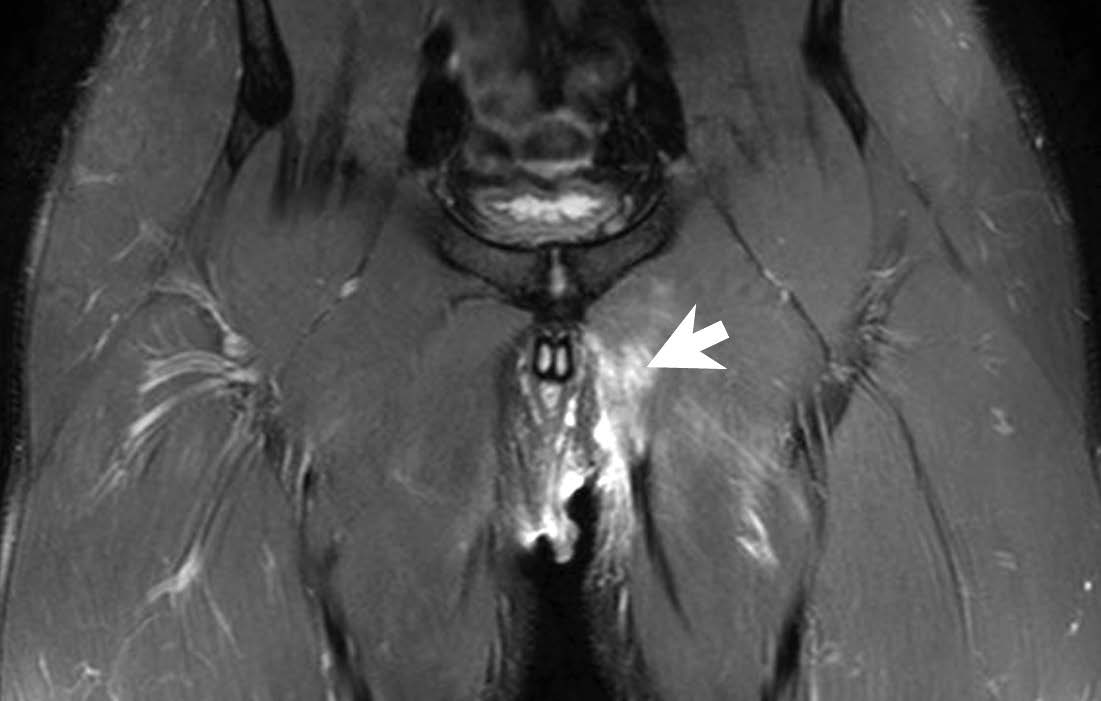
Figure 3: MRI imaging shows a grade 1 partial muscle tear of the left adductor longus muscle and tendon at the superior pubic ramus insertion with fl uid (1.5cm wide) along the superfi cial fascia.
The risk of injury when playing futsal is lower than playing soccer.This is due to stricter rules in futsal.For example, in futsal, slide tackles are prohibited. Players are recommended to stop the ball by chesting the ball rather than heading it. This can help prevent head and neck injuries.1,2
Although there are fewer futsal injuries than soccer injuries there are typical injuries seen in futsal. Junge A and Dvorak J4 analyzed player injuries during three consecutive futsal world cups. There were a total of 165 injuries from 127 matches, or 130 injuries per 1,000 player matches. The majority of injuries were caused by contact with other players and 35% occurred during non-contact with other players. Most injuries affected the lower extremities (70%), head and neck (13%) and upper extremities (10%) and trunk (7%). The most frequent injuries were contusions of the lower leg (11%) ankle sprains (10%) and groin strains (8%). These were caused by contact with other players and by foul play.
The most recent futsal world cup was held in Thailand in November 2012. There were only three serious injury cases reported from all matches, with other less serious injuries reported, including minor strains and abrasions. Futsal injuries are mainly caused by contact with the ground or other players. To prevent fractures of the lower extremities, shin pads and straps are essential to protect the lower thigh, knee and ankle.
In the FIFA Futsal World Cup Thailand 2012, Brazil defended their title, winning it for the fifth time by defeating Spain. All the players who experienced serious injuries during the tournament were attended by the BASEM center of the Bangkok Hospital. The injuries involved two cases of grade 1 and one case of grade 2 leg muscle tears which responded well to conservative and symptomatic management. BASEM is an accredited FIFA medical center of excellence.









