Electronic ISSN 2287-0237
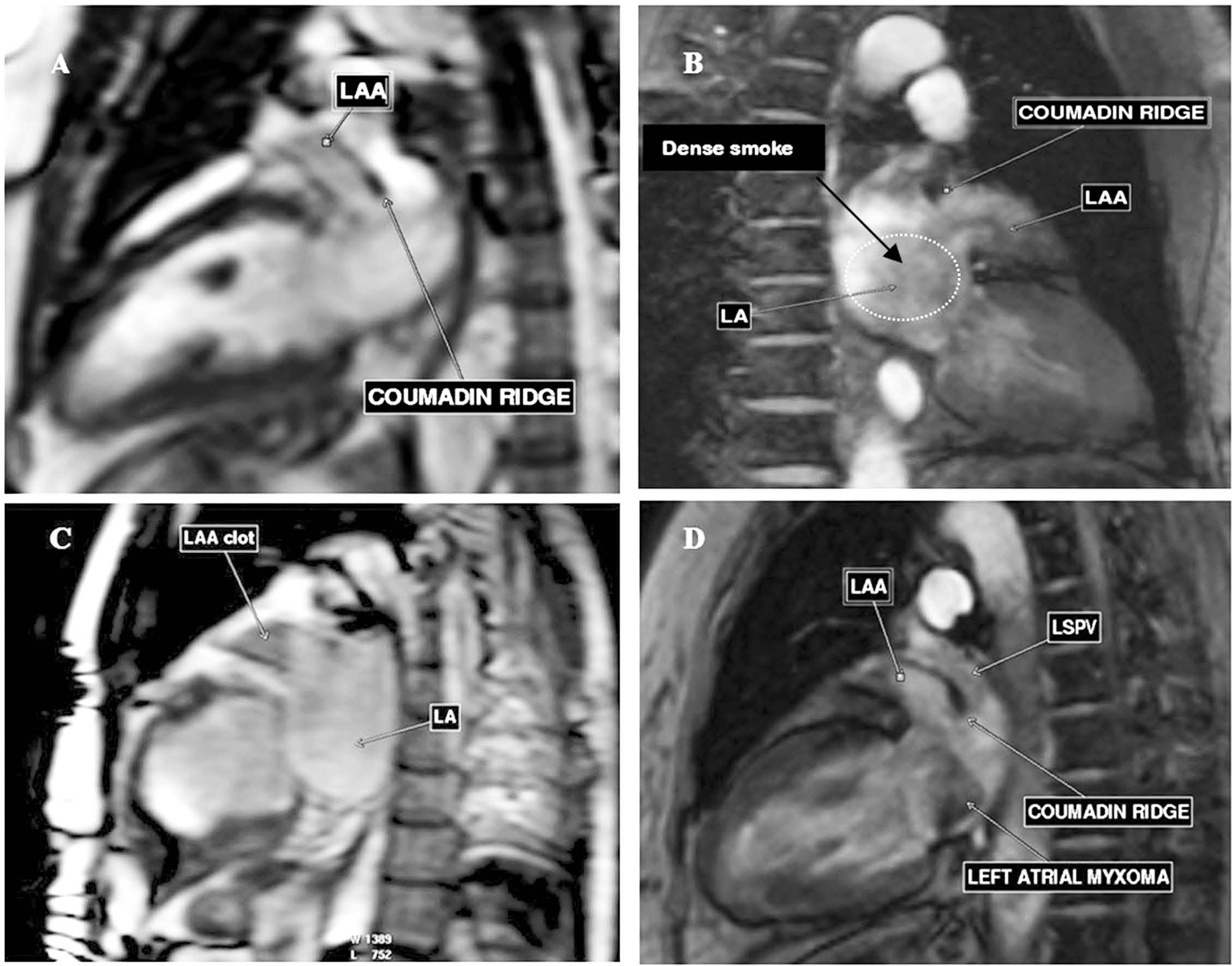
(A) The CINE MRI image on vertical long axis view shows the band-like structure of coumadin ridge in the LA in between the LAA mouth and emptying port of the LSPV.
(B) The CINE MRI image on vertical long axis view shows a bulbous protrusion at the tip of coumadin ridge in the dilated, dense smoke left atrium.
(C) The CINE MRI image on vertical long axis view shows LAA clot.
(D) The CINE MRI image on vertical long axis view shows the left atrial myxoma that obstructs the mitral inflow.
The coumadin ridge is considered to be a pseudo- tumor that exists between the left atrial appendage and the emptying port of the left superior pulmonary vein. It may be misdiagnosed as a thrombus or a cardiac tumor.1 This ridge is named “coumadin ridge” because it is always be diagnosed as a thrombus that brings the patient to be treated with anti-coagulant (coumadine/ warfarin) unnecessarily. Furthermore, the coumadin ridge is also an essential part for imaging as the inter-atrial septum, the left atrial appendage (LAA) and the left superior pulmonary vein (LSPV) in patients with atrial fibrillation (AF).2
The coumadin ridge is smooth muscle ridge and in fact it is a fold of the lateral left atrial wall protruding into the endocardial surface of the left atrium. Therefore, the coumadin ridge is also called the left lateral ridge (LLR).3 The coumadin ridge is the atrial tissue that separates the entrance of the left superior pulmonary vein and the left atrial appendage. The coumadin ridge is usually thin in the proximal part and can be bulbous at the distal part. This makes the coumadin ridge looks like a cotton-tip applicator or “Q” tip sign visualized on the transesophageal echocardiogram. The distal tip of the coumadin ridge may be large and can protrude into the left atrium and left atrial appendage that make it looks like a clot or small tumor. The narrow coumadin ridge is found to be less than 5 mm between the LSPV and the LAA in the majority of patients3 and the cross section of its narrowest part shows the round contour in the majority (75%), flat in 15% and pointed in 10% of cardiac specimens.2 The unique position of the coumadin ridge is between the os of the left atrial appendage and emptying port of the left superior pulmo- nary vein.4 The coumadin ridge is not a pathologic disease but it is a normal variant of the cardiac structure and is not a consequence of coumadin administration. The structural components of the coumadin ridge are the vein or ligament of Marshall, autonomic nerve bundle and small atrial artery or may be a sinoatrial node artery.2 The ligament of Marshall is the remnant of the superior vena cava and lies along the epicardial aspect of the ridge. The ridge has muscular connections with the left pulmonary vein and these connections can be a triggering substrate of focal atrial fibrillation.5 In previous studies, the coumadin ridge has been used as a catheter ablation site.6 The size and contour of the coumadin ridge is important information that can determine the effectiveness and safety of AF catheter ablation. In the case of the pointed shape coumadin ridge, accidental injury of the PV during AF ablation must be considered, ablation is recommended to stay on the LAA side of the ridge.
The most common left atrial masses to be differentially diagnosed from the coumadin ridge are; (i) thrombus, (ii) tumors in the left atrium (LA) such as atrial myxoma. The structural characteristic and especially the location are the important clues to specify the coumadin ridge. The common location of the left atrial thrombus is the left atrial appendage (LAA) and the LA thrombus is often associated with atrial fibrillation. More than 90% of left atrial thrombi are detected in the LAA.7 Atrial myxoma is the most common cardiac tumor and about 75% occurs in the left atrium. Atrial myxomas are almost always single but sometimes they may be sessile or peduculated and attached to the inter-atrial septum in the region of fossa ovale.8 The LA thrombi and the left atrial myxoma often cause the obstruction of blood flow but the coumadin ridge does not.9
The Coumadin ridge is almost always accidentally observed on diagnostic images when assessing for blood clots in the left atrial appendage. Transthoracic echo- cardiography (TTE), transesophageal echocardiography (TEE) and MRI are common tools for left atrial clot screening. To demonstrate a blood clot, the coumadin ridge and tumor need an imaging background that is contrast- able to these pathologies. When using MRI, the intensity of the coumadin ridge, blood clot and some cardiac tumors have a similar intensity. Hence the unique location of the coumadin ridge in between the LAA and the LSPV will be an important clue to specify the ridge. The spin echo MRI with black blood pulse sequence imaging may not help in coumadin ridge identification because the back- ground signal is almost similar to the coumadin ridge. Gradient echo MRI pulse sequence provides the bright blood image that can be used to project the ridge. Contrast injection may not be necessary to be used for imaging the ridge but may be helpful to identify the organized blood clot or tumor in the left atrial appendage and in the left ventricle. A gradient echo CINE MRI image on vertical long axis view is recommended to be used to image the coumadin ridge. The LAA, the coumadin ridge and the left superior pulmonary vein are also well demonstrated together on this CINE image view (Figure A-D). Gradient echo CINE MRI provides structural information including the mobility format of the LA ridge, LA clot and LA tumor in the same image. When the coumadin ridge is prominent it may be seen as a Q tip sign on the images of both echocardiogram and MRI. The severely slow blood flow or dense smoke that moves around the coumadin ridge in the markedly dilated and poor contraction left atrium in cases of chronic AF creates more spontaneous contrast background in the left atrium that makes the coumadin ridge look like it’s blooming and bigger than usual which is easily observed on gradient echo CINE MRI images.
In our experience at the Bangkok Heart Hospital, we always use MRI as a screening tool to rule out LAA clot for pre-Atrial Fibrillation (AF) ablation preparation and before cardioversion if the patient has no contraindications for MRI scanning. This is because MRI has high spatial resolution and no angle limitation and also provides the good contrast background to the LA mass. In the case of AF catheter ablation, the coumadin ridge becomes an important part to be identified as well as any blood clots in the LAA and left atrium structure.
The coumadin ridge itself is not a pathologic condi- tion but it is a normal variant structure in the left atrium. However, the existence of the coumadin ridge must be known to avoid misdiagnosis as a thrombus or tumor. The unique location and structure of the coumadin ridge are the most helpful clues to confidently differentiate the coumadin ridge from the other diseases that occur in the left atrium. The accurate identification of the coumadin ridge and its characteristics must be emphasized as important as the inter-atrial septum, the left atrial append- age and the left superior pulmonary vein in patients with atrial fibrillation.









