Electronic ISSN 2287-0237
Diffuse large B-cell lymphomas (DLBCLs) is the most common subtype of non-Hodgkin lymphoma (NHL).1 In Thailand, DLBCLs accounts for 67% of NHL.2 The cancer behaves aggressively with heterogeneous outcome. Several prognostic and predictive factors have been used in clinical practice for DLBCLs, including Ann Arbor staging,3 International Prognostic Index (IPI),4 age-adjusted IPI,5 International Extranodal Lymphoma Study Group (IELSG) risk score,6 and cell of origin (COO), which is either germinal center B-cell (GCB) and non-GCB.7,8 Studies in the last decade demonstrated that double-hit B-cell lymphomas have poorer prognosis than those without double-hit.9,10 The Revised WHO Classification of Lymphoma 2016 includes “high- grade B-cell lymphoma (HGBL), with MYC and BCL2 and/or BCL6 rearrangement” as a new subtype of B-cell lymphoma.11 Some studies have showed that the detection of protein expression by immunohistochemical study (IHC) is comparable to molecular study of gene rearrangement; however, this method has not yet been accepted to classify this subtype of lymphoma.12-14 MYC/BCL2 expression is the most important because it accounts for the majority of lymphoma with double expression and is associated with poorer prognosis in patients with DLBCLs.13,14
The prevalence and the prognostic value of MYC/BCL2 double expression has not been studied in Thailand. Therefore, this study was conducted to report the prevalence of DLBCLs with MYC/BCL2 double expression and to determine whether it has effect upon survival.
Abbreviation
Patients
In this retrospective observational study, 88 patients diagnosed with DLBCLs according to the WHO Classification 2008 criteria1 at King Chulalongkorn Memorial Hospital (KCMH) from 2013 to 2014 were retrieved. Eight patients with incomplete clinical data were excluded from the survival analysis.
Methods
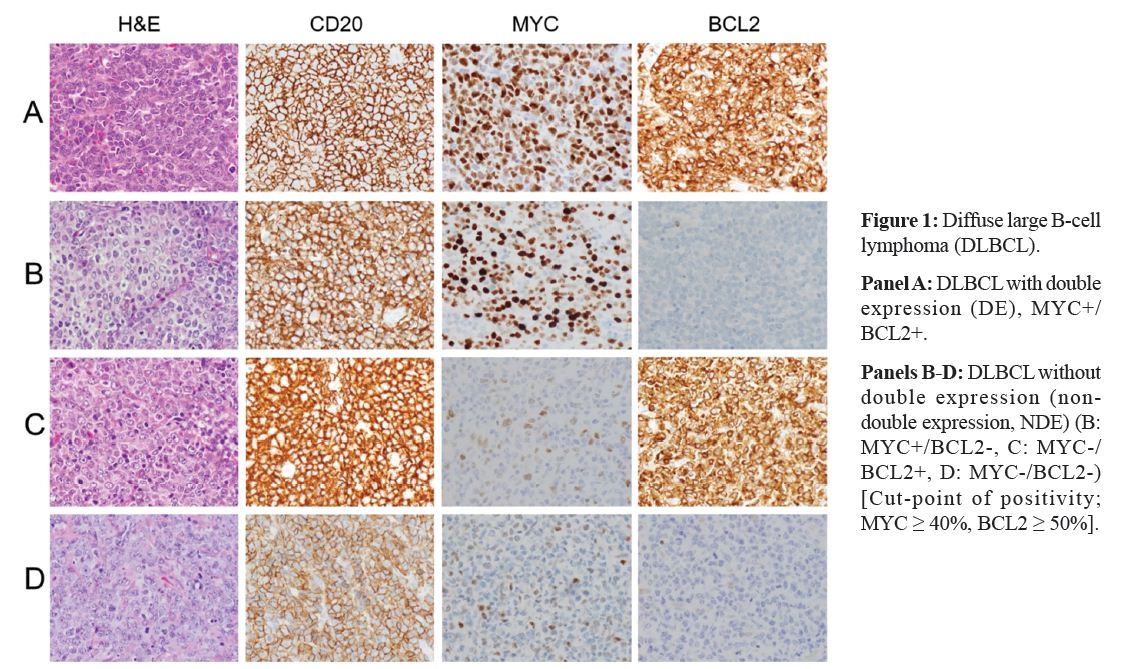
Histologic slides of all cases were reviewed. MYC and BCL2 immunostains were performed on formalin-fixed paraffin-embedded sections, using anti-c-MYC (Y69) rabbit monoclonal primary antibody (Ventana®), and monoclonal mouse anti-human BCL2 oncoprotein clone 124 ready-to-use (Dako®), respectively. The percentage of MYC and BCL2 was separately assessed by two pathologists, CP and TA. The positive cutoff values of MYC and BCL2 according to the WHO Classification of lymphoid neoplasm 2016 were ≥ 40% and ≥ 50%, respectively (Figure 1). Cases with discordance of positive/negative interpretation were reviewed together to reach a consensus. For the remaining cases with concordant interpretation, the mean percentage of positive cells was used for further analysis. The clinical data of all patients were collected from the medical records. The follow-up period was 2 years. The overall survival (OS) and progression-free survival (PFS) were recorded. This study was approved by the Institutional Review Board, Faculty of Medicine, Chulalongkorn University, and number 613/59.
Statistical Analysis
Qualitative data were recorded as frequency and percentage. Differences in categorical data were analyzed by Chi-squares test or Fisher’s Exact test. Continuous data were recorded as mean and standard deviation, and were compared by t-test. Kaplan-Meier survival curve was used to demonstrate the median survival time. The difference of median survival time was analyzed using Log-rank test. Multivariate analysis was also implemented to detect possible confounders. Then, Cox proportional hazard model was used to calculate the hazard ratio and the adjusted hazard ratio. The effect modification was analyzed, using multivariate analysis and log-likelihood ratio test with p < 0.10 as the cutoff point for statistical significance. This part used Stata/IC 12.1. Other results were displayed as number with 95% confidence interval (CI) and were considered statistically significant if p < 0.05.
The prevalence of MYC/BCL2 Double Expression (DE)
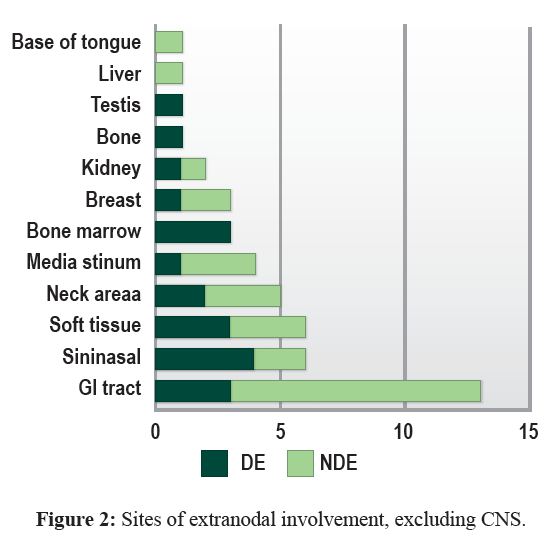
There were 88 patients diagnosed with DLBCL from 1 January 2013 to 31 December 2014; all of which were included in the prevalence study. Fifty-two (59%) cases were biopsy specimens and 36 (41%) cases were excisional specimens. Extranodal non-CNS sites, lymph node, and CNS accounted for 46 (52%), 25 (29%) and 17 (19%) cases, respectively. The most common site of extranodal involvement was the gastrointestinal tract, 13 cases (15%) (Figure 2). There were 36 (40.9%) male and 52 (59.1%) female patients. The mean age was 60±16 years old (range, 17-94 years). Five (6.25%) of patients had HIV infection. Forty (46.6%) cases were found to have DE of MYC/BCL2.
Clinical characteristics of the patients included in the survival analysis
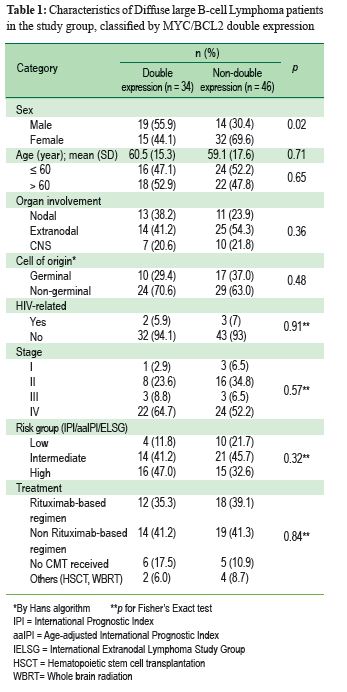
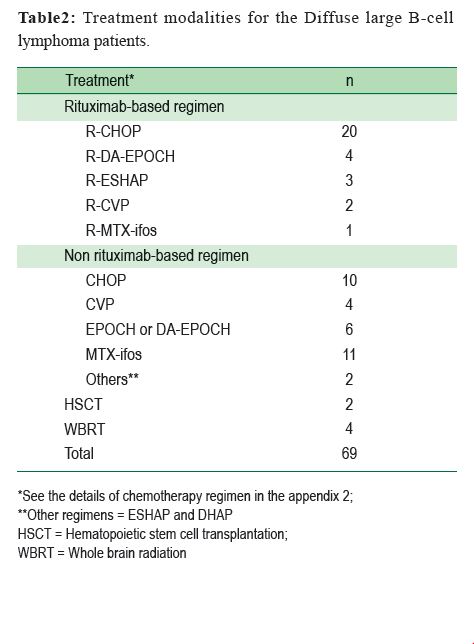
Eight patients were excluded from the analysis of survival due to incomplete clinical data; 6 from the double expression (DE) group, and 2 from the non-double expression (NDE) group. The remaining 80 patients were divided into two groups, DE and NDE. The patients’ characteristics are listed in Table 1. There was no significant difference between the two groups except for sex, i.e., there were significantly more male patients in the DE group than in the NDE group. The detail of the treatments is shown in Table 2. Eleven patients did not receive chemotherapy because of death before 1 month of follow-up time in 6 cases, end of life care in 2 cases, loss of follow-up in 2 cases, and referral to another hospital in 1 case.
 The Overall Survival (OS), Progression-Free Survival (PFS) and Hazard Ratio (HR) of DE group compared to the NDE group
The Overall Survival (OS), Progression-Free Survival (PFS) and Hazard Ratio (HR) of DE group compared to the NDE group
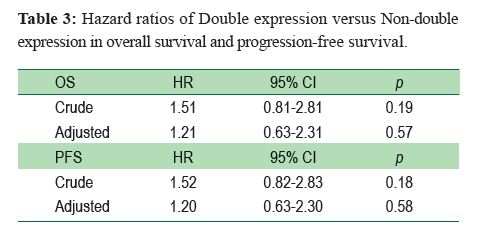
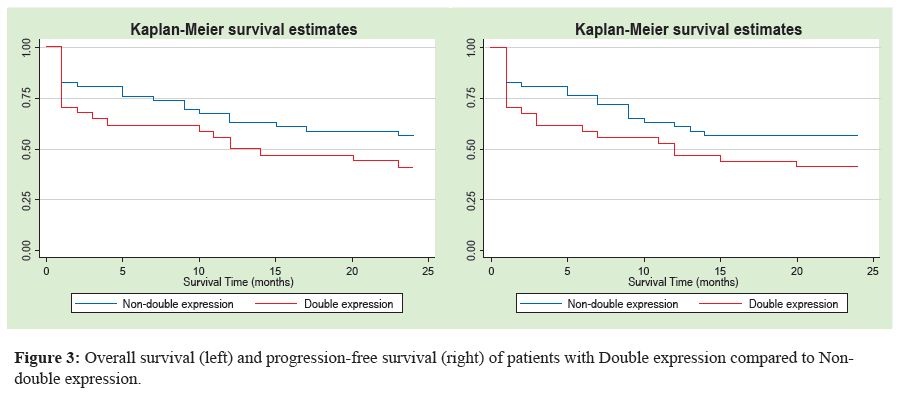
At the end of follow-up (2 years), 40/80 patients had died. Twenty patients who passed away were in the DE group (58%) and the remaining 20 were in the NDE group (43%). Both OS and PFS are shown in Figure 3. The median OS time was shorter in the DE group (14 months vs. 24 months, Log-rank test, p = 0.16). Multivariate analysis found that sex, COO, risk group and treatment were the confounders. The adjusted HR was 1.21 (95%CI 0.63-2.31, p = 0.57). The median time of PFS was also shorter in the DE group (13.5 months vs. to 24 months, Log-rank test, p = 0.16). The adjusted HR was 1.20, (95%CI 0.63-2.30, p = 0.58). All of them were not statistically significant (Table 3).
Effect modification and its interaction with hazard ratio
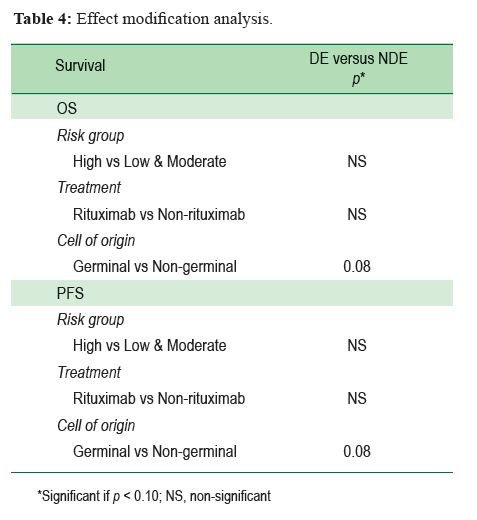
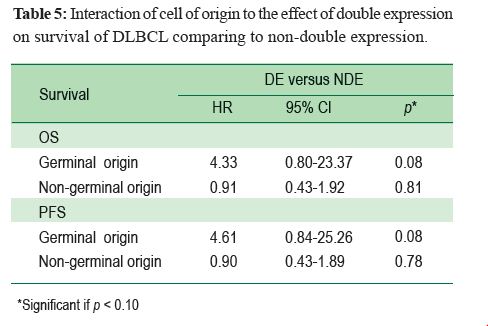
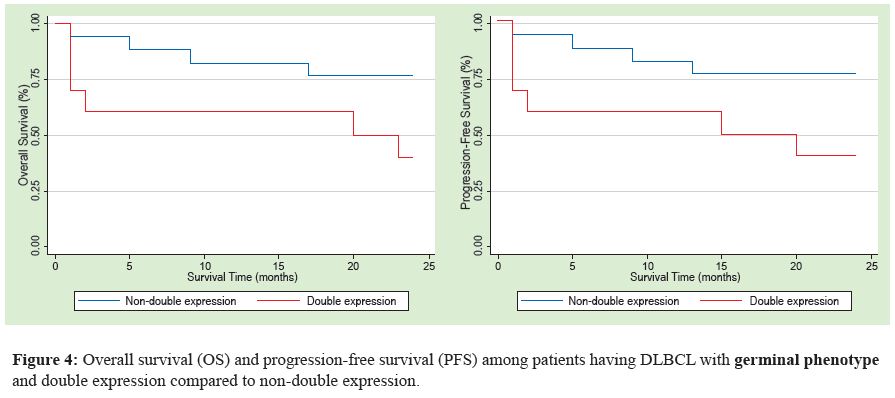
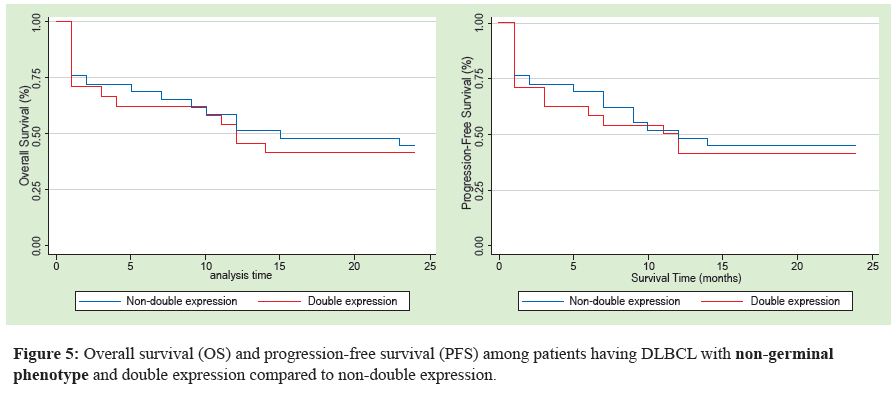
The effect modification of COO, risk group and treatment was done. COO had statistically significant interaction with the HR of both OS and PFS (Table 4). In GCB phenotype, the DE group had a HR of 4.33 (95%CI 0.80-23.37, p = 0.08, significance level of p < 0.10) for OS, and 4.61 (95%CI 0.84-25.26, p = 0.08, significance level of p < 0.10) for PFS. In the non-GCB phenotype, the HR was not statistically significant (Table 5, Figure 4 and Figure 5).
To the best of our knowledge, double expression of MYC/BCL2 has not been reported in DLBCLs in Thailand. In our cohort of Thai patients, the prevalence of DLBCL with double expression is 46.6%. This figure is higher than those observed in the United States of America (21%)13 and Denmark (19%)14 but it is within the range of the Chinese population (30-60%).15,16 Primary CNS lymphomas tend to be non-GCB phenotype, which is more common to have double expression.17 Therefore, one reason that could be attributed to the difference between our prevalence and the Western prevalence is the inclusion of primary CNS DLBCLs to our study (7 DE and 10 NDE; 7 GCB and 10 non-GCB phenotypes). Ethnicity is also another factor that could play role in the differences.
In our study, there were significantly more male patients in the DE group, compared to the NDE group. This might represent selection bias due to small population or an association between DE and sex, which has not been described. Besides gender, other patient characteristics are not significantly different. Some of the previous reports excluded HIV patients from their studies13,14,18 while some did not mention the HIVstatus.15,16 5 cases (6.25%) of our patients were HIV-infected, and such a small proportion had no statistical significance, both as a confounding variable and an effect modifier. Although all of the studies so far have found no effect of DE on the prognosis of patients with DLBCLs, the significance of DE among HIV patients has not yet been explored in a large cohort.
The DE group tended to have worse OS and PFS, as well as adjusted HR for both risk of dying and risk of having progression, but all of these were not statistically significant. Our findings are contradictory to the results of previous
studies.13,14 This could be due to the smaller population and shorter follow-up duration of our study; the previous cohorts that found DE to be significantly associated with worse prognosis enrolled at least 100 patients with a period longer than 3 years of follow-up. A future study with a larger number of patients, longer duration of follow-up and a multicenter study might provide more accurate information. In addition, the prevalence of high grade B-cell lymphoma with double hit of MYC and BCL2 rearrangement in Thai patients and whether or not double expression can predict the presence of double hit remains to be investigated.
From the effect modification model, there is an interesting result with regards to the cell of origin in our cohort. Among those with GCB phenotype, patients with DE were 4.3 times more likely to die and 4.3 times more likely to have progression than those with NDE. Among patients with non-GCB phenotype, the risks of dying and the risk of having progression were similar in both groups. This result is different from the finding of The International DLBCL Rituximab-CHOP Consortium Program in which DE had poorer prognosis in the non-GCB subgroup.18
Sesques and Johnson19 recently reviewed DLBCLs and high-grade B-cell lymphomas (HGBL) and their correlation with DE, double hit (DH) and mechanism of gene rearrangement of MYC and BCL2. They demonstrated that most DLBCLs with DE and GCB phenotype have DH caused by gene translocation, which is the same mechanism of DH in HGBL. Therefore, some DLBCLs with GCB phenotype and DE are in fact HGBL. This could explain why DE has poorer prognosis among patients with GCB phenotype. Furthermore, FISH for MYC and BCL2 translocation should be performed in
DLBCLs with GCB phenotype and DE because it is the most cost-effective method to identify patients with DH-HGBL. This suggests that, in addition to the cell of origin, DE should be considered as one of the important biological risk factors that should be included in the pathological report.
The prevalence of MYC/BCL2 double expression DLBCLs seem to be higher in Thai patients compared to American and Danish, but comparable to Chinese. Double expression alone was not statistically associated with prognosis in our cohort. However, for the GCB phenotype subgroup, those with DE carried poorer outcome.









