Electronic ISSN 2287-0237
Thailand is a developing country that is moving away from agriculture to industrialization. Due to the rapid development with expansion of economics, society, education and communication, Bangkok has become one of the cities with air pollution, especially particulate matter less than 10 microns (PM10) and particulate matter less than 2.5 microns (PM2.5), which is caused by automobile exhaust especially diesel,1 smoke from burning wood and factories.2-7 Air pollution problems affect people’s health, especially causing respiratory diseases.
The results of previous epidemiological studies by both Thai and foreign researchers showed that there was a relationship between exposure to PM2.5 and health effects in both the short-term and long-term, causing diseases such as asthma, chronic lung inflammation, deterioration of lung function, respiratory tract infection and lung cancer. PM2.5 can be deposited in the respiratory tract more easily than larger particles.8-12 Not only the size of particulate matter affects mortality and morbidity but also the concentration and components.13 However, these will vary according to activity and the environment.14 In addition, many studies indicated that some microbial agents such as bacteria and fungi affect the respiratory system. Kurup V et al.15 in 2000 showed that fungi in the air were associated with allergy and asthma. There were 4 - 11% of fungi contaminants in PM2.5.16 Besides, the correlation of microbials in the air and particulate matter showed that PM2.5 and PM10 in the summer and autumn would be higher than other seasons.17 Most of the fungi were found in PM 2.1- 3.3.18
Boonchoo W.19 in 2005 studied the effects of PM10 on the pulmonary function of street sweepers. In this study, researchers specifically studied the microbes that sweepers could be exposed to during work shifts, becauses there was a lot of fine particulate matter, bacteria and fungi spread during sweeping. Moreover, they were working near the roadside which was a risk of PM2.5; and the emissions from vehicles. Therefore, we aimed to study the concentration of PM2.5, bacteria and fungi that may affect the respiratory symptoms and pulmonary function of the sweepers.
Samples selection
One hundred and ninety people were sweepers at Rajthevee district. They worked three shifts per day. The first shift operated by 100 sweepers was in the morning from 05.00 am to 01.00 pm; the second shift operated by 80 sweepers was in the afternoon from 01.00 pm to 09.00 pm; and the last shift operated by 10 sweepers was at night from 09.00 pm to 05.00 am. Rajthevee district had several places which were sources of particulate matter less than 2.5 microns and microbes such as hospital, skytrain, a street market, construction and heavily trafficked roads. The study group was selected from the sweepers working in the morning shift at Rajthevee District in Bangkok. The method was to follow up the activities of the sweepers who had worked more than 3 months at Rajthevee district in Bangkok (Figure 1), the sweepers who were not currently sick or admitted in hospital, the sweepers who worked by sweeping the road and who volunteered in this study. So, a number of 97 sweepers at Rajthevee District in Bangkok participated in this research.
This study was accepted by the Review Committee of the CHEST 2012 Annual Meeting in Atlanta on July 09, 2012.
Sampling and analysis
Collection of PM2.5
The samples of PM2.5 were collected during February-June 2011 using Polytetrafluoroethylene (PTFE) filters (Model 225-1709, SKC Inc. USA), the filters were equilibrated on desiccators in the controlled room for 24 hours before and after sample collection.

Figure 1: Shows 50 districts of Bangkok, Thailand. Rajthevee district is highlighted in red.
The temperature for this room was 20-23°C (± 2°C) and the relative humidity was 30-40% (± 5% RH). The Model 200 Personal Environmental Monitor (PEM™) was attached to the sweepers’ collar near the breathing zone with a personal sampling pump (Gilair 5/Gilian, USA). The personal sampling pumps were calibrated using DryCal DC-lite at flow rate 4 L±20 ml/min. The time average for sampling was about 6 hours during the work shift. Each filter was weighed by using a microbalance (METTLER Model UMT-5) before and after sampling collection.
The concentration of PM2.5 in micrograms/m3 was cal- culated as follows:
C = Ms/ Vs
C = concentration of PM2.5, μg/m3
Ms = mass of PM2.5, μg
Vs = the volume of air sampled, m3
Collection of microbial agents
Microbial air samples were collected during February- June 2011 using Microflow 90 (Aquaria, Italy) following the sweepers twice a day at 06.00-07.00 am and 10.00-11.00 am. Microflow 90 was calibrated by the calibrator at a flow rate of 30 L/min, volume 100 L. Four percent of Sabouraud dextrose agar was used for collecting fungi and plate count agar was used for collecting bacteria. After collecting samples, plates with agar were incubated at a suitable temperature for bacteria and counted within 48 hours and fungi was counted within 5 days.
The concentration of microbial was calculated as follow:
Measuring pulmonary function
The sweepers’ pulmonary function at the end of their work shift was measured using a spirometer (DATOSPIR 120 Model D, Spain). The sweepers were informed and a demonstration was made by the researcher before the test. The Thoracic Society of Thailand’s guideline of pulmo- nary function test was used.
In addition, the general characteristic and respiratory symptoms questionnaires were used in this study. A chest specialist and occupational medic audited the question- naire before being used.
Testing Serum IgE
The sweepers with wheezing were selected for testing serum IgE.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, version 16). Chi-square test or Fisher’s exact test was used for analyzing any association between PM2.5, bacteria and fungi with respiratory symptoms. Pearson correlation was used for analyzing the association between PM2.5, bacteria and fungi with pulmonary function test.
Concentration of PM2.5 and microbial
The samples of PM2.5 and microbial were collected from 97 sampling sites at Rajthevee district. The average concentration of PM2.5 was 373.72 μg/m3 (SD = 165.35). A total of 194 air samples were collected for investi- gating bacterial counts and 194 air samples were col- lected for investigating fungal counts. It was found that the mean of bacterial counts at 06.00-07.00 am was 885.83 cfu/m3 (SD = 264.69), and at 10.00-11.00 am was 741.90 cfu/m3 (SD = 245.92). The mean fungal counts at 06.00-07.00 am was 620.37 cfu/m3 (SD = 215.01), and at 10.00-11.00 am was 462.79 cfu/m3 (SD = 202.73).
Respiratory symptoms
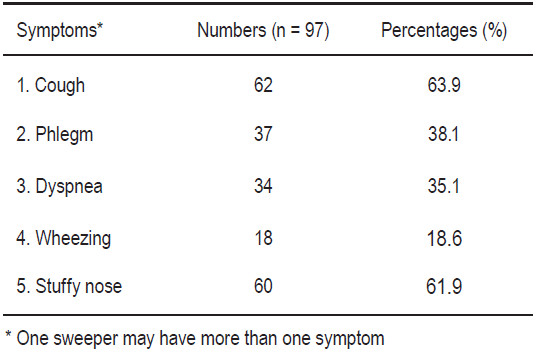
The respiratory symptoms of sweepers in this study were classified into five symptoms. The results were shown in Table 1.
Table 1: The respiratory symptoms of the sweepers
The 95 sweepers were tested for pulmonary function at the end of work. Only two sweepers could not be tested because one person was post-operative for a stomach surgery and another one had had a motorcycle accident. The values from the spirogram were FVC (Forced Vital Capacity), FEV1 (Forced Expiratory Volume in one second), FEV1/FVC ratio and FEF25-75% (Forced Expiratory Flow at 25 - 75% of FVC). The classification of the severity pulmo- nary function impairments were graded into 4 levels as shown in Table 2. The interpretation of pulmonary function impairment was classified into two patterns: restrictive disorder as found in 33 workers (97.06%) and obstructive disorder as found in 1 worker (2.94%).
The association between PM2.5 and microbes with respiratory symptoms
The association of PM2.5 and microbes with respiratory symptoms was analyzed using Chi-square test or Fisher’s exact test. The PM2.5 was associated with stuffy nose (p < 0.01), and associated with cough (p < 0.05). The data is shown in Table 3. The fungi at 06.00-07.00 am were associated with wheezing (p < 0.05). The data is shown in Table 4. There was no significant association between bacteria and respiratory symptoms.
The association between PM2. 5 and microbes with pulmonary function.
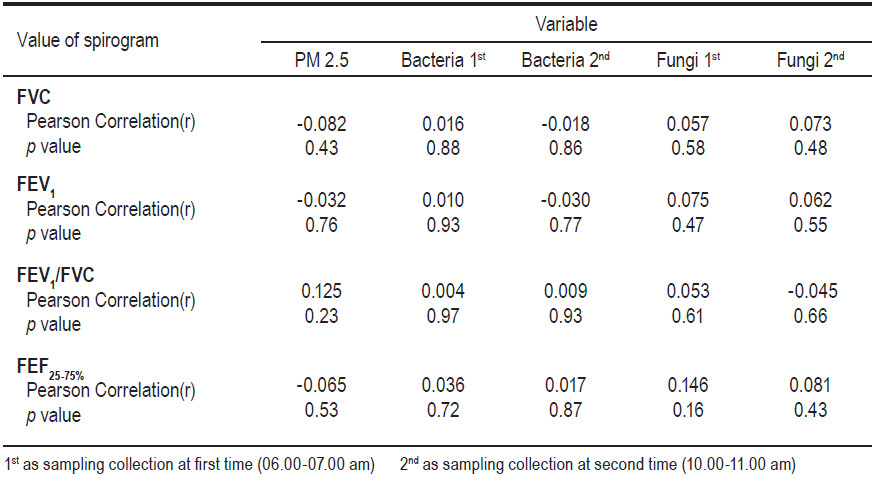
There was no significant association found between PM2.5, bacteria and fungi with a pulmonary function test in sweepers. The data is shown in Table 5.
Table 2: Classifi cation of the severity of pulmonary function impairment (n= 95)
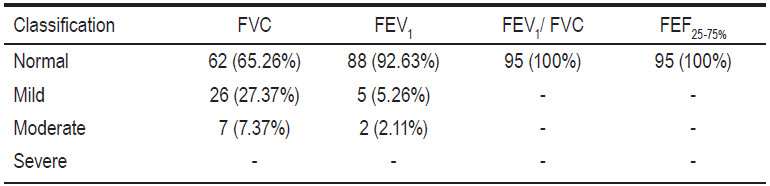
Table 3: The association between concentrations of PM2.5 and respiratory symptoms (n = 97)
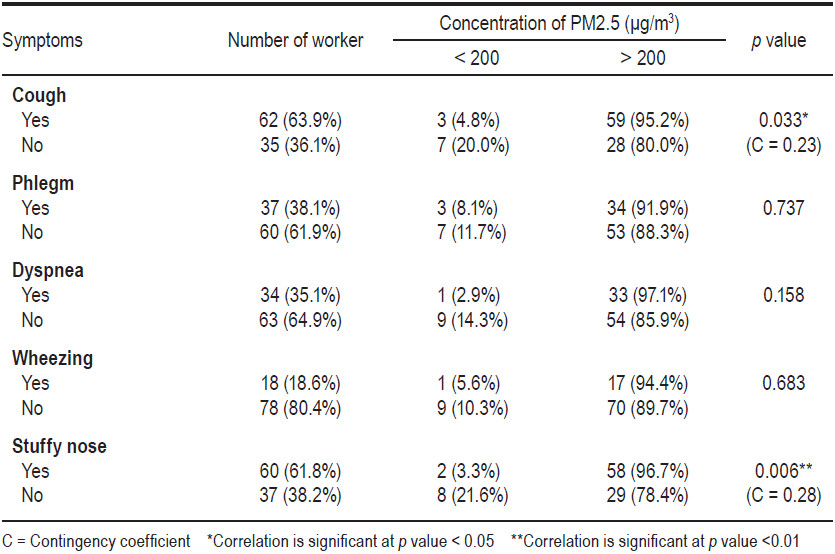
Table 4: The association between concentrations of fungi and respiratory symptoms (n = 97)
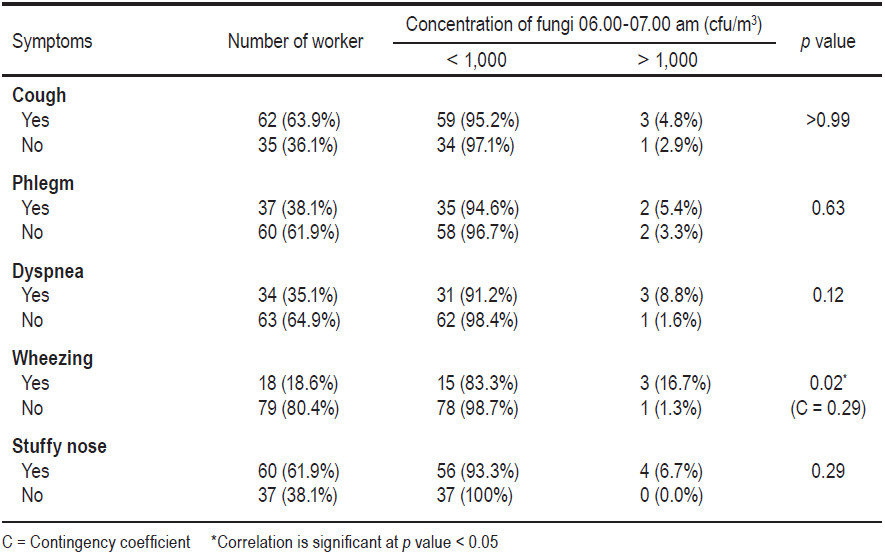
Table 5: Correlation between concentrations of PM2.5, bacteria and fungi with pulmonary function of sweepers by Pearson correlation.
Serum IgE
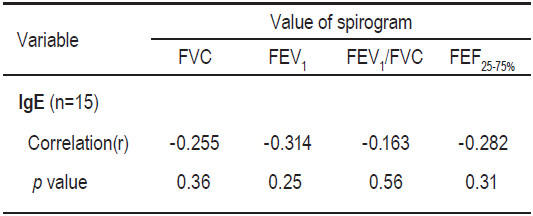
Among 15 sweepers who had wheezing, the mean of IgE levels was 277.07 IU/ml (range 12-1,088 IU/ml). Nine sweepers were more than the standard of 100 IU/ml. There was a correlation between poor pulmonary function and increased IgE levels.
The concentration of PM2.5 was different in each street area of the sweepers. This might be caused by different traffic conditions, environment, construction, trading on the street and the place to rest during working (for example, sweepers rested during work near an intersection, under expressway, store, bus stop, or in a building). Wang G et al.20 in 2002 assessed concentra- tions of PM2.5 at 6 sampling site in Nanjing. The average concentration of particulate matter 2.5 was 481.4 μg/m3, the most concentrations of particulate matter 2.5 were found at heavy traffic areas. Bacteria and fungi were mostly found in the area of heavy traffic and crowded areas with lots of street venders. The dusty road was similar to the one studied by Luksamijarulkul P and Kongtip P.21 in 2010 who analyzed the microbial count and particulate matter of 10 microns on roadside areas under skytrain sta- tions in Bangkok. The highest concentration was at the Victory Monument area that had many people and heavy traffic.
The association of PM2.5 and microbes with respiratory symptoms was not found. Perhaps the sweepers used a veil or mask during work and worked during certain periods of time by sweeping the streets twice per work shift, and not sweeping continuously all day. This may have explained the few respiratory symptoms in sweepers. Morgenstern V et al.22 in 2007 studied respiratory health and individual estimated exposure to traffic-related air pollutants in a cohort of young children in the city of Munich, Germany. Significant associations were found between the pollutant PM2.5 and sneezing, runny/stuffed nose during the first year of life (OR 1.16, 95% CI = 1.01 to 1.34) that was similar to the effects observed for the second year of life. Patel MM et al.23 in 2010 studied concentration of black carbon and PM2.5 with respiratory symptoms in high school students in New York City and found that increments of black carbon were associated with increased wheeze, shortness of breath, and chest tightness. However, concentration of PM2.5 was not consistently associated with increment of symptoms. Mopuang M.24 in 2005 studied concentration of PM10 and microbial count with respiratory symptoms among street vendors in Bangkok Fashion City found that the prevalence of air quality related to illnesses in studied street venders was 58%. It was shown that 28% had eye irritation symptoms, 16.67% had shortness of breath and/or sore throat, and 10.67% had running nose symptoms. The relationship between studied factors including bacterial counts and PM10 and air quality related to illnesses was analyzed, and showed no significant association (p > 0.05).
Manystudiesshowthatexposuretofine particulate matter would affect lung function.25-30 However, our study pro- posed to test the association between the concentration of PM2.5 and microbial agents with pulmonary function in sweepers by the Pearson correlation test and it showed statistical significance. But the duration of work was associated with pulmonary function in sweepers. This might be due to the sweepers having worked twice a day in work shifts (not continuously) and that they were protected by using a mask during sweeping. It might be that pulmonary function would be affected in the future if the sweepers are exposed to fine particulate matter and microbial agents for a longer time with high concentration. The study of Gotschi T et al.31 in 2008 assessed FEV , FVC and the ratio of (FEV /FVC) for 9 years in following up adults from 21 European centers.
Fine particles (PM2.5) were measured in 2000/2001 using central monitors. The result found no significant associations between city-specific annual mean PM2.5 and average lung function levels. The study of Pawaree in 2004 found no association between inhalable dust and pulmonary function of sugar mill workers. In this study, there was correlation between poor pulmonary function and increased IgE levels (Table 6). Sherrill DL et al.33 in 1999 studied total serum IgE and its association with asthma symptoms and allergic sensitization among children in USA. The result showed that both persistent wheezing and early sensitization were associated with high serum IgE levels at all ages. Shadick NA et al.34 in 1996 studied the relationship of serum IgE level and the rate of decline of pulmonary function in Boston. The result also showed that an increment of levels of serum IgE was associated with lower levels of pulmo- nary function.
Table 6: Correlation between serum IgE levels with pulmonary function of sweepers by Pearson correlation.
show a relationship with pulmonary function impairment among sweepers. We may need to perform a longitudinal study. We recommend to select and use personal protective equipment that could effectively protect the workers as well as finding a method to reduce the particulate matter in ambient air.
Acknowledgements
This study was partially funded by the Center of Excellence on Environmental Health, Toxicology and Management of Chemical (ETM) under the Science & Technology Postgraduate Education and Research Development Office (PERDO) of the Ministry of Education. The authors would like to thank the Public Cleansing and Public Park Section of Rajthevee District, Bangkok, and staff of the Environmental Quality and Laboratory Division of Pollution Control Department.









