Electronic ISSN 2287-0237
A cut appendicitis is one of the most common causes of acute abdominal pain. Some cases present as classical right lower quadrant pain and tenderness. Serum blood test findings include elevation of white blood cells (WBC), neutrophil and C-reactive protein test. However other cases may present with other more unusual symptoms and in these situations a computed tomography (CT) image and/or pelvic ultrasonic scan is recom- meded to provide additional support to the diagnosis.
The normal appendix diameter size is not more than 6 mm, and the mural wall is 2 mm thick. The common locations are retroceacal, pelvic and retroileum, and other locations are subceacal, preileal, and extraperitoneal (in 5% of reported cases). The other associated findings are periappendiceal edema with or without fluid collection. Fecalith in situ is most likely reported in the diagnosis. This case report gives details of three cases of acute appendicitis with differing presentations.
A 9-year-old male presented with the chief complaint of fever, abdominal pain for 3 days, vomiting for 8 hours and one bout of diarrhea prior to admission. Physical examination (PE) revealed lower abdominal pain and decreased bowel sounds. Total WBC 55.96*10^3/mm3 (normal range 4.5-13.0 *10^3/mm3), neutrophil is 87.2% (normal range 46.5-75.0%). CT image without contrast enhancement and oblique reconstruction at right lower abdomen reveals an enlarged appendix 2 cm in diameter with an edematous mural wall with periappendiceal edema (Figure 1A). A single, small fecalith is seen at the root of the appendix. The tip of the appendix points to the pelvic cavity. Pelvic ultrasonic scan reveals an enlarged appendix 2 cm in diameter with thickening mural wall (Figure 1B). Pathological diagnosis is acute necrotizing appendicitis, ruptured (Figure 1C).
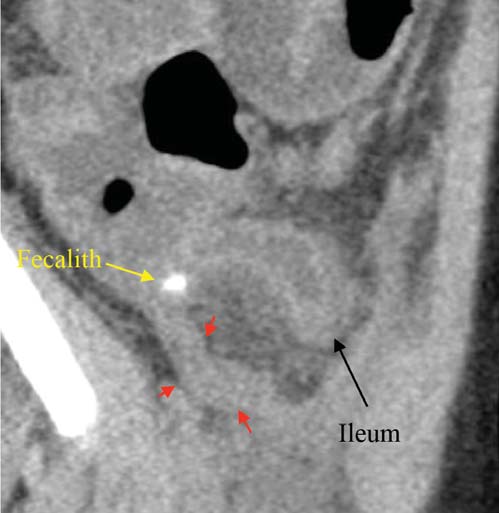
Figure 1A: CT image reveals markedly enlarged appendix with thickening wall (see red arrows).
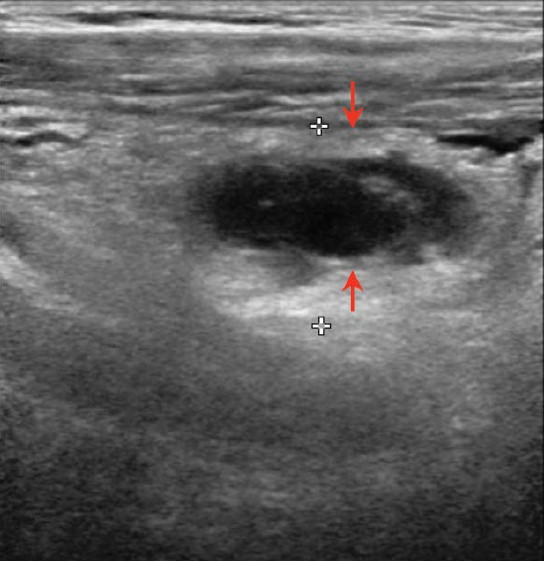
Figure 1B: ultrasonic scan finding reveals enlarged appendix with thickening wall (see arrows).
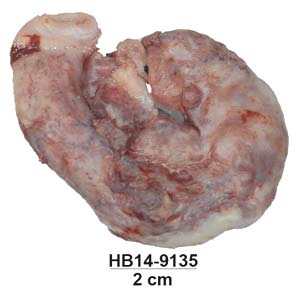
Figure 1C: Gross specimen of appendix.
A 41-year-old male presented with the chief complaint of abdominal pain with diarrhea for 2 days and one day of fever and persistent abdominal pain.(PE) reveals marked tenderness at the right lower quadrant (RLQ), otherwise findings are unremarkable. Total WBC is 11.22 *10^3/ mm3 (normal range 4.0-10.0*10^3/mm3), neutrophil is 86% (normal range 46.5-75.0%).
CT image without contrast enhancement on the sagittal section reveals swelling of the appendix with a thickening mural wall containing a fecalith, located at the retrocecal region (Figure 2A). There is periappendiceal edema surrounding the body of the appendix. Pathological diagnosis is acute suppurative appendicitis with severe serositis, with presence of a fecalith (Figure 2B).
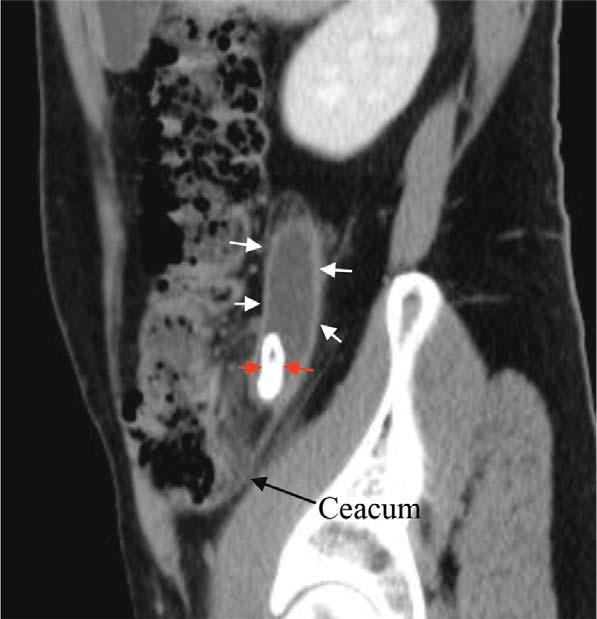
Figure 2A: CT image reveals enlarged appendix (see white arrows) containing calcified fecalith (see red arrows).

Figure 2B: Gross specimen of appendix with fecalith.
A 22-year-old female presented with the chief complaint of acute colicky abdominal pain, no fever or diarrhea is observed. PE tenderness at epigastrium and mid abdomen otherwise findings appear unremarkable. Total WBC 9.1 *10^3/mm3 (normal range 4.0-10.0 *10^3/mm3), neutrophil is 76.43 (normal range 46.5-75.0%). CT image reveals an enlarged appendix behind the terminal ileum (Figure 3A).
Pelvic ultrasonic scan reveals enlarged appendix with a thickening mural wall and minimal free fluid near the tip of the appendix, the terminal ileum lies anteriorly (Figure 3B). Pathological diagnosis show acute suppurative appendicitis with periappendicitis (Figure 3C).
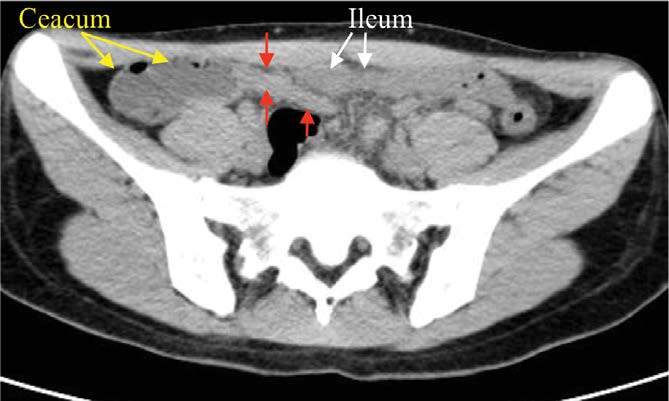
Figure 3A: CT image reveals enlarged appendix behind terminal ileum (see red arrows)
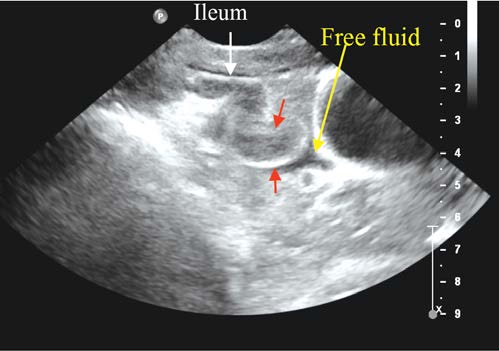
Figure 3B: Ultrasonic scan reveals enlarge appendix with a thickened mural wall (see red arrows)
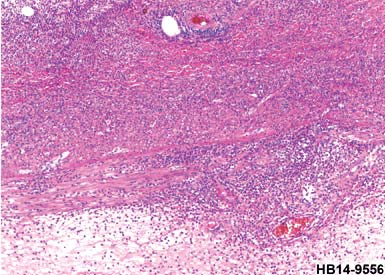
Figure 3C: Microscopic scan shows acute suppurative appendicitis with periappendicitis
These three cases of acute appendicitis are presented with CT image findings, and in some cases diagnosis was obtained in combination with a pelvic ultrasonic scan to show the common locations of appendicitis to include the pelvic, retroceacal and retroileal regions. It is important to know the precise appendiceal location for surgical planning. The use of CT image and ultrasound are excel- lent in diagnosis with high sensitivity and specificity. The appendix can be found by tracing the tubular structure that arises from the tip of the ceacum. There are some evidence-based issues about the optimization of using im- age modalities in this condition. A recent meta-analysis3 reveals CT examination in adult patients has high sensitiv- ity and specificity for acute appendicitis and is superior to ultrasound with graded compression. But in the pediatric group, graded compression ultrasound is highly sensitive and specific in detecting acute appendicitis.
In equivocal cases, ultrasound followed by CT exami- nation has a higher sensitivity but lower specificity than ultrasound alone because of increased false positives.
In case of suspected pregnancy, ultrasonic scan should be the first diagnostic tool employed, and in some cases, it may be complicated to detect an enlarged appendix. On an ultrasonic scan we have to strictly identify each element, especially the ceacum and ileum. The other possibility is colonic diverticulitis. The CT image plays an important role here mainly at the ceacum and ascending colon. In diverticulitis, opaque density at the colonic wall may be depicted and is associated with evidence of pericolonic edematous changes.
CT image and /or pelvic ultrasonic scan should examine the appendiceal locations and size of appendix with clinical correlation as well as laboratory findings in the diagnosis of acute appendicitis. Samples are presented with imaging and gross specimen/microscopic scans.
Ultrasonic scan is the first priority in case of pregnancy, and the identification of the ceacum and ileum are an important consideration. The other possibility to investigate is colonic diverticulitis with shown the depiction of opaque density at the colonic wall and evidence of pericolonic edematous changes may also be observed.









