Electronic ISSN 2287-0237
Since the Thai economy and society changed from an agricultural society to an industrial society, workers have made their migration into the cities to work and earn a living. As a result, the older adults and children are abandoned to stay at home, or the older adults have to stay home alone.1 Moreover,the family structure has also changed from the extended family to the nuclear family.2 This leads to an increasing number of older adults living alone. The current trend of older adults living alone increased from 3.6% in 1994 to 6.3%, 7.7%, and 8.6% in 2002, 2007, and 2011, respectively.3 Older adults living alone at home are considered to be a major risk group to have health problems, both physical and mental. Common physical health problems in older adults are mostly chronic diseases such as hypertension, diabetes, bone and joint problems and heart disease.4 It also leads to a risk of infection, falls and death at home.5,6 For mental health problems, it was found that many older adults feel lonely, desperate7 and discouraged. The perceived mental health was lower than those who live with family members.8 They also have dementia, depression, and even suicidal thoughts.9-11 In terms of social issues, this group of older adults runs a high risk of social isolation as they have less interaction with others, less power, low self-esteem,12 and experience a lack of social support and networks. This can lead to inappropriate behaviors which can cause physical and mental health problems.13,14
Since leaving older adults to live alone may cause many of the health problems mentioned above, self-care behavior is very important to this group because they have no family members to provide care and assistance. Al- though the results of the research in other countries have mainly revealed that living alone as an older adult does not mean facing loneliness there is more of a risk of health problems than older adults who live with their families.15-17 Yet, this group of older adults living alone feel that they have a better health status than those who live with others.17 It is clear, therefore, that there are some inconsis- tencies in the studies. Also, most research and studies are studied in other countries which have different cultures. In some western countries, living alone for older adults is more commonplace and the government plays a major role in providing welfare for older adults. However, in Thailand, taking care of an older adult is the responsibility of the family. But, at present, the trend of taking care of older adults has been decreasing,1 and from the reviews of research in Thailand, there have been no studies associated with social isolation and the links among the perceived social isolation, self-care behaviors and health status of older adults living alone in the community. Therefore, in order to prepare for Thailand’s aging society and the increasing number of older adults living alone in the country, the researchers were interested in this issue in order to provide guidelines for the development of improved health care and quality of life for older adults living alone.
This study was a descriptive correlational analysis research. The samples were the community dwelling older adults aged 60 and over living alone in Muang District, Sa Kaeo Province, Thailand. The study was conducted from April to June 2015. The inclusion criteria included:1) living alone for at least six months, 2) being able to speak and understand Thai language and not having communication problems, and, 3) no impairments in thinking and memory, based on Chula Mental Test.18 The score obtained from the test must be equal to or greater than 15 points. Through purposive sampling, samples of 212 participants were recruited to the study.
The sample size of the study was calculated with the level of significance (α) equal to 0.05, the power of test equal to 0.80, and the effect size equal to 0.20, which was a small effect size. The two-tailed test was used to calculate the sample size using the G* Power 3.0.10 Program.
The research instruments included 4 questionnaires as follows:
Part 1: The demographic characteristics questionnaire. This was used to gather the general information of the samples. The questionnaire was in the form of multiple choices and open-ended questions. It consisted of 20 questions, including the information of gender, age, marital status, education, income, health problems and information about living alone.
Part 2: The perceived social isolation questionnaire. The test created by Cornwell and Waite14 was used. The test was translated into Thai and the back translation process was used. The test consisted of 9 questions with two aspects: the aspect of the feeling of isolation which was 3 negative questions and the perceived social support which was 6 positive questions. A three-point Likert Scale was used for the answers. In terms of scoring, for a negative question the points were distributed as: never (1 point), sometimes (2 points) and often (3 points). For a positive question the points were distributed as: never (3 points), sometimes (2 points) and often (1 points). The scores ranged from 9-27 points. The interpretation of the scores was divided into three levels: low perceived social isolation (score < 14), moderate perceived social isolation (15-20 points) and high perceived social isolation (score > 21).
Part 3: The questionnaire of self-care behaviors. The self-care behaviors were assessed by using the self-care behaviors assessment in older adults which was created according to the concept of Orem by Waraporn Thingerd.19 It consisted of 22 items, including:
A five-level Likert Scale was used. Seventeen items were positive questions. In terms of scoring, the points ranged from: not performing at all (0 point), to regularly performing (4 points). There were 5 items of negative questions, and in terms of scoring, the points ranged from: not performing at all (4 points), to regularly performing (0 point). The score ranged from 0-88 points. The inter- pretation of the scores was divided into three levels: poor self-care behaviors (score ≤ 52), fair self-care behaviors (53-69 points) and good self-care behaviors (score ≥ 70).
Part 4: The questionnaire of perceived health status assessment. The Short Form -36 Health Survey (SF 36) (Version 2) which was developed by Ware et al.,20 and translated into Thai by Jirarattanaphochai et al.21 was used. There were 36 questions with two health dimensions: 21 items of physical health and 15 items of mental health. The interpretation of the score depended on the types of questions in each subscale. For example, for the questions on physical functioning, the points ranged from: greatly reduced (0), slightly reduced (50), and not reduced (100). For mental health, the points ranged from: always (0), mostly (25), sometimes (50), once in a while (75), and never (100). Then the points were put together and the average point of each subscale was calculated. After that, the average point of each subscale was put together as the component. The scores ranged from 0-400 points. The interpretation of the scores was divided into three levels: low perceived health status (0 -133.33 points), moderate perceived health status (133.34-266.67 points) and high perceived health status (266.68- 400 points). The contents of the questionnaires were verified by 3 experts, namely 2 experts in geriatric care and an expert in community health and family nursing. The questionnaires were improved before piloting with 15 subjects whose charac- teristics were similar to those of the subjects in the main study. After that, the reliability of the perceived social isolation, self-care behaviors and perceived health status questionnaires were analyzed by using Cronbach ‘alpha coefficient. The reliability of the questionnaires was 0.83,0.84 and 0.94 respectively.
Protecting the rights of the samples: The researcher submitted the consent to do research on people to the Human Research Ethics Committee of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University. It was approved with Approval No. 2015/118 to protect the rights of the samples from the process of gathering data to the presentation of the findings. Participants were informed of the purpose of the research and given details about the activities as were the samples. The samples were also informed that they could leave the study at any time.
Data collection
Muang District, Sa Kaeo Province was selected specifically as it is the largest and the most populated district in the province. Stratified random sampling was used to identify potential partipants as there are 8 sub- districts in Sa Kaeo and the Sa Kaeo Sub-district is the largest the most populated sub-district. So it was chosen as a representative sample of a big sub-district to study. Also, one small sub-district was selected from seven sub-districts by simple random sampling: drawing lots. Khok Pi Khong sub-district was selected. So, there were two sub-districts in total. The name lists of 315 older adults living alone were categorized, and divided into three groups based on age: 60-69 years, 70-79 years and 80 years and over. After that the numbers of samples required based on the ratio for each group was calculated. The numbers of the older adults in each group were 84, 88 and 40 people, respectively. Then a simple random sample by drawing lots was administered and 212 samples were obtained. Also, the process of data collection was done.
Data analysis
The data were analyzed by a Statistical Package. Descriptive statistics, including the frequency, percentage, mean and standard deviation were analyzed. Pearson’s Product Moment Correlation and chi-square were utilized to determine the relationships of the variables.
It was found that most of the samples were females (76.4%), and almost half of them aged 70-79 years (41.5%). The average age was 72.34 years (Min = 60, Max = 93, SD = 7.78). The samples were mostly Buddhists (98.2%). They were widowed (72.6%), and single (8.5%). More than half of them completed primary school level (69.8%) and did not work (64.6%). The average income was 3991.48 Thai baht. The source of income was from their children (51.4%). Most of them had health problems (76.9%).
The first top three health problems were hypertension (57.7%), arthritis / joint problems (55.8%) and hyper- lipidemia (38.0%), respectively. For the period of living alone, it was 5-10 years (35.4%). Regarding the reasons for living alone, more than half of them were living alone after the death of their spouses, and their children worked in other areas and had their own families (69.3%). Half of the samples had negative feelings towards living alone (53.3%), including feeling lonely and bored, followed by feeling neutral (25.0%). However, 21.7% of them had a positive feeling towards living alone as they felt free and had privacy, and they also were proud to take care of themselves. Most of them were not worried about being alone (75.0%), whilst a smaller proportion of them were concerned about it (25%). The matters of concerns included fear of illness without close supervision, fainting, falling, and crime. Most of them did not have difficulties living alone (75.9%).
More than half of the samples perceived social isolation as medium (62.7%) while 12.7% of them perceived it as high. Half of the samples had a fair level of self-care behaviors (55.2%) and a perceived physical health status that was relatively high (50.5%), and more than half of them perceived their mental health status as high (60.8%). Education and income were correlated with the perceived social isolation and were statistically significant. The chi-square was equal to 6.194, p = 0.045 and 17.489, p < 0.001, respectively as shown in Table 1. Gender, education and income were associated with self-care behaviors and were statistically significant. The chi-square was equal to 9.288, p = 0.01, 10.255, p = 0.006 and 21.414, p < 0.001, respectively, while income and health problems associated with physical health status were statistically significant. The chi-square was 14.584, p = 0.001, 9.726, p = 0.008, respectively. Finally, income linked to mental health status was statistically significant with a chi-square of 23.309, p < 0.001.
Table 1: The links among basic factors (gender, marital status, education, income and health problems) and perceived social isolation of older adults living alone in the community by chi-square (n = 212).
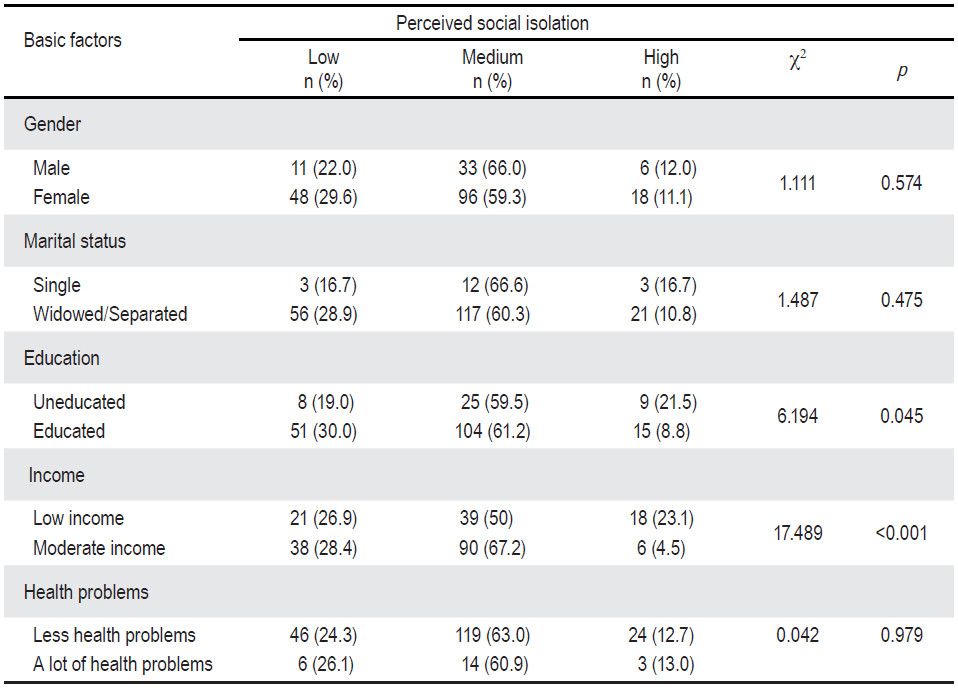 Table 2: The links among age, perceived social isolation, self-care behaviors, physical health status and mental health status among older adults living alone in the community using statistical Pearson’s Product Moment Correlation (n = 212).
Table 2: The links among age, perceived social isolation, self-care behaviors, physical health status and mental health status among older adults living alone in the community using statistical Pearson’s Product Moment Correlation (n = 212).
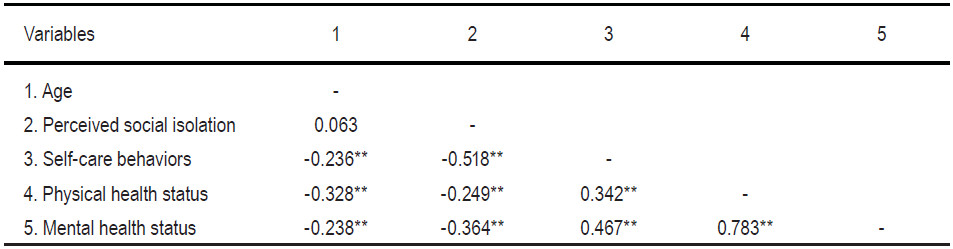
The perceived social isolation of negative links with self-care behaviors, physical health status and mental health status were statistically significant: r = -0.518 (p < 0.001),r = -0.249(p < 0.001) and r = -0.364 (p < 0.001), respectively. Self-care behaviors were positively associated with physical health status and mental health status and were statistically significant: r = 0.342 (p < 0.001) and r = 0.467 (p < 0.001), respectively. Age was negativelyassociated with self-care behaviors, physical health status and mental health status and were statistically significant:r = -0.236 (p < 0.001),r = -0.328 (p < 0.001) and r = -0.238 (p < 0.001),respectively,as shown in Table 2.
The results of the study revealed that more than half of the samples had moderate perceived social isolation. This can in part be explained because some of them were supported by their children in terms of needed resources, especially money although their children did not live with them. Moreover, the samples also received psychological and emotional support from the persons who were close to them. They still had relatives and friends / neighbors. So, they might not feel very lonely. Half of the samples had self-care behaviors at a fair level and more than half of them had perceived physical health status and mental health status at a high level. It might be because most of them were early and middle older adults, whose physical and mental health, awareness and intelligence was not in bad condition. So, they had the capacity for self-care and were still healthy.22
It was also found that basic conditioning factors were associated with perceived social isolation, self-care behaviors and health status. Income had a negative corre- lation with the perceived social isolation and was statisti- cally significant. This can be partly explained as income was a factor that allowed older adults to access resources without having to rely on others. So, they were proud of themselves. This was in accordance with the study of Parkotwong W.12 in 2008 which found that income was associated with loneliness among older adults living alone. It was also found that income was associated with self-care behaviors and health status and this was statisti- cally significant since having sufficient income or a good economic status allowed individuals to access more health resources, and they were likely to be healthier than those who earned less.23 This was consistent with the findings of the study of Zhou et al.24 in 2015 which revealed that the elderly with low incomes were associated with poor health status.
Regarding education, it was associated with perceived social isolation and this was statistically significant. Those who were educated obviously had communication channels and social networks. They had social support to ascertain needed information to be applied as a solution or relief of the problem that people were facing.25 Therefore that could result in those who were better educated to have a lower perceived social isolation than those who did not get education. It was also found education was associated with self-care behaviors and this was statistically signifi- cant since education gave individuals the skills and oppor- tunities to communicate with others and have increased access to health information. As a result, they had good self-care behaviours.23 In this study, older adults who had received education had better self-care behaviors than those who did not, which was in accordance with the study of Bai et al.26 in 2009.
Age was negatively associated with self-care behaviors and this was significant statistically as an increasing of age was an indication of the deterioration of physical health, resulting in the reduction of the ability in taking care of themselves without support from others. The results of the study also revealed that age was negatively associated with perceived health status and this was statistically significant. This was consistent with the study of Smith and Goldman27 in 2006 which was found that age was negatively correlated with the perceived health of the elderly. However, there was no correlation between age and perceived social isolation. This may be because the elderly had adequate social support from their children, relatives and friends / neighbors. This was consistent with the study of Hawthorne.28
Gender was associated with self-care behaviors and this was statistically significant. In this study, the majority of the samples which were females had better self-care behaviors than males. This was because the role of the females was determined as the persons providing care to others. So, they had experience and skills in self-care. They were also sensitive to changes and tried to keep themselves in a healthy condition.29 This was consistent with the study of Khwandao Klamrat30 in 2011. Nevertheless, gender was not associated with perceived social isolation. This may be because most of the female respondents were early and middle older adults who had the ability to participate in social activities, so they can gain social supports and work for a living. This allowed them to have better self-esteem and they felt less lonely and isolated.12 This was consistent with the study of Hawthorne28 in 2008, which was found that gender was not associated with perceived social isolation.
Marital status was not associated with perceived social isolation, self-care behaviors and health status. This was probably because most of the samples were widowed as their spouses passed away and some of them were single. So, they were all considered as not having spouses. This was consistent with the study of Dale et al.31 in 2011, which found that marital status was not associated with self-care behaviors and health status of older adults living alone.
Health problems and perceived health status were correlated and were statistically significant. Illnesses caused difficulties to individuals, families and society, and health status and perceived health status of individuals influenced management of illnesses.22 Thus, health problems of the samples were obviously associated with perceived health status. This was consistent with the study of Caetano et al.32 in 2013. However, their health problems were not associated with the perceived social isolation. This was probably because health problems did not impede social activities. The samples were treated at the Health Promoting Hospital near their homes, so they met with friends who had similar health problems, and they could exchange experiences.8,15 This allowed the samples to perceive that having chronic diseases or health problems was common with older adults.
The links among perceived social isolation, self-care behaviors and health status and perceived social isolation and self-care behaviors were negatively correlated and this was statistically significant. It can be explained according to the theory of Orem that those who have interactions with society will be supported in the future, so they can take care of themselves the way that society does. If people, however, have a sense of isolation and lack the ability to socially interact with others, they will lack the ability to care for themselves and have inappropriate self-care behaviors.22 This was in accordance with study of Bai et al.26 in 2009, which revealed that self-care behav- iors were negatively correlated with feelings of loneliness and depression, but there was a positive correlation with social support.
Perceived social isolation and health status were negatively associated with each other with a statistical significance. This is best described by the concept of Cornwell and Waite14 in 2009 that the causes of social isolation of persons are chronic diseases and physical, mental, social and intellectual deterioration, which lead to the lack of social networks and less social support. This will affect the physical and mental health of individuals.14 This was in accordance with the studies of Cornwell and Waite14 in 2009, and Hawthorne28 in 2008, which found that older adults with high perceived social isolation usually had links with poor physical and mental health.
Self-care behaviors and health status were positively correlated. It can be explained by the concept of Orem that promoting and maintaining health status are the results of ongoing care. This is done deliberately with a targeted and structured process. When it is done effectively, it will contribute to well-being and health and people can perform their duties effectively. It can be said that health status is a result of self-care.24 The results of this study were consistent with the study of Sunsli et al.33 in 2012, which revealed that self-care behaviors were correlated with health status.
According to the results of this study, it can be concluded that there were links among perceived social isolation, self-care behavior and health status of older adults living alone in the community. Thus, in assessing the health status of older adults, these factors should be taken into account, especially in older adults who have low income and are uneducated. The access to health services and social services should be increased and offered served to reduce perceived social isolation. Encouraging older adults to have good self-care behaviors based on an individual basis will help older adults living alone in the community to have both good physical and mental health. This will result in a better quality of life.
We would like to express our gratitude to the director of Sa Kaeo Crown Prince Hospital, the community nurses, the health care officers, the community leaders and the sample participants who facilitated, cooperated and gave their time to take part in this study.









