Electronic ISSN 2287-0237
To report midterm results and assess clinical markers which can predict intramyocardial angiogenic cell precursors (ACPs) injection for cardiomyopathy outcomes.
Between May 2005 and April 2010, 143 consecutive cardiomyopathy patients underwent intramyocardial ACPs injection. Sixty patients were dilated cardiomyopathy (DCM) and 83 were ischemic cardiomyopathy (ICM). Mean age was 59.6 ± 12.1 years. ACPs were isolated from patient’s own blood and cultured. Number of cells prior to injection was 47.3 ± 36.8 million cells. ACPs were injected into non-viable myocardium and hypokinetic segments. Combined coronary artery surgery and cell injection were performed in 34.9% of ICM. Kaplan-Meier was used to estimate survival time. Cox proportional hazard model was applied by fitting data which included age, gender, diagnosis, diabetes, hypertension, hypercholesterolemia, pulmonary hypertension, renal failure, NYHA class, serum creatinine, preop LVEF, type of operations and number of ACPs into the model to identify predictors of death.
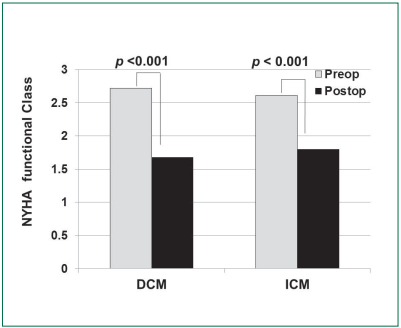
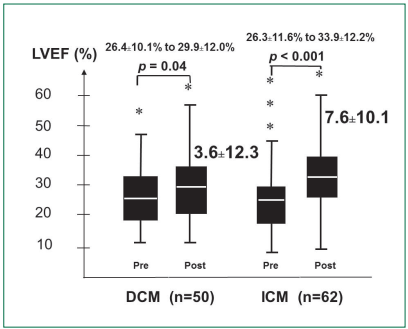
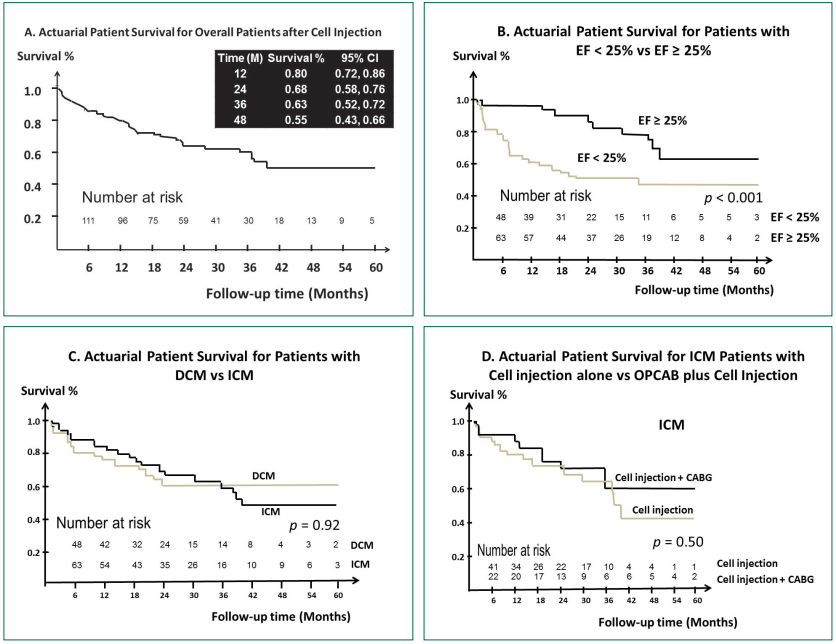
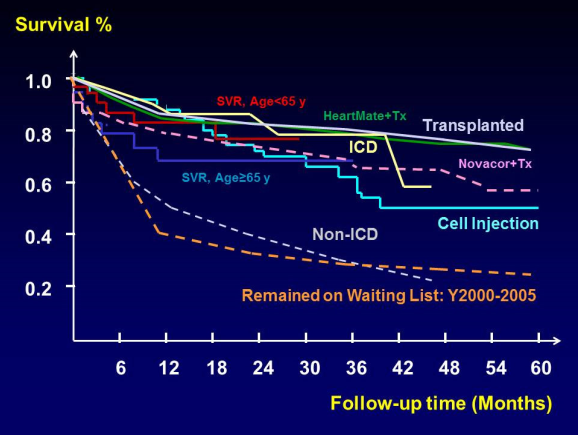
There was no new ventricular arrhythmia. Thirty-day mortality rate was 3.3% (2/60) for DCM and 8.4% (7/83) for ICM. Overall death rate was 14.5/1000/month (95%CI: 10.6-19.5). Overall survival probability at 12, 24, 36 and 48 months was 79.9% (95%CI: 72.1-85.8), 67.9% (95%CI: 58.5-75.6), 62.9% (95%CI: 52.4-71.7), 55.4% (95%CI: 43.0-66.2), respectively. LVEF improved by 3.6±12.3% (p = 0.04) for DCM and 7.6±10.1% (p < 0.001) for ICM. ICM patients with combined coronary artery surgery and cell injection showed more LVEF improvement. (11.8±11.6% vs 4.9 ± 8.0%, p = 0.007). Cox regression analyses suggested only preop LVEF (hazard ratio 0.91, 95% CI 0.87-0.95, p < 0.001) was associated with decreased survival.
Intramyocardial ACPs injection improved LVEF in both DCM and ICM. Preop LVEF was a signifcant survival predictor.
10.31524/bkkmedj.2017.02.003