Electronic ISSN 2287-0237
Shoulder injuries are one of the most common problems faced by competitive athletes. A shoulder dislocation is a serious complication, and more than 95% of all shoulder injuries are anterior dislocations. Furthermore, the recurrent dislocation and subluxation are common complications after a traumatic shoulder dislocation. Conservative treatment is not sufficient to prevent future complications. An aggressive investigation and early surgical correction is called for as the best approach to achieve promising future results.1
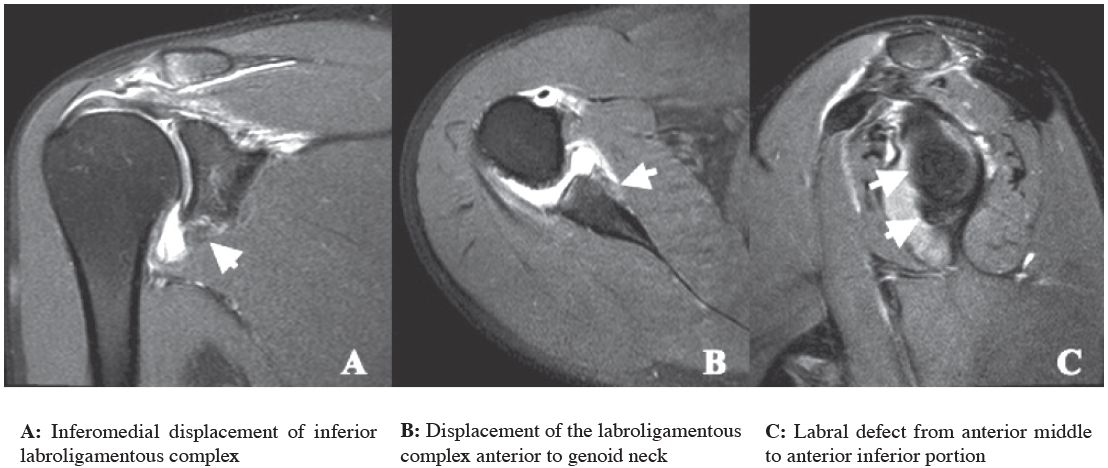
A 28-year old man fell and sustained a blunt injury to the right shoulder. He had primary treatment at a local hospital, and one and a half months passed before he came to the Bangkok Academy of Sports and Exercise Medicine (BASEM) department at Bangkok Hospital. The magnetic resonance image (MRI) for arthrography rendered an excellent depiction of a localized labral injury. It was decided that an arthroscopic repair would be performed at the site of this major injury, with a shorter tear in-operation. The MRI arthrogram (see Figure A-C) revealed a tear of the anterior middle to anterior inferior labrum, inferomedial displacement of the inferior labroligamentous complex anterior to the glenoid neck and an osseous defect at the posterior portion of the humeral head. The findings were compatible with anterior labroligamentous periosteal sleeve avulsion (ALPSA) and Hillsach deformity. The athroscopy of the right shoulder revealed a right glenohumeral subluxation anteroinferior subluxation, a Bankart and an ALPSA lesion. The arthoroscope via an anterior glenoid approach was used to perform a Bankart and ALPSA repair.
The glenohumeral joint has a rather wide range of movement, wider than any joint in the body. It is the most common dislocated joint due to its small and shallow glenoid fossa.2,3 The ALPSA is a main factor of shoulder instability.4









