Electronic ISSN 2287-0237
Erectile dysfunction (ED) was previously defined by the term “impotence” with a very broad encompassing meaning including the lack of sexual desire. The definition of erectile dysfunction was revised in 1993 to be more accurate, pertaining to individuals who desire but fail to perform sexual activity because they could not achieve or maintain an erect penis long enough to obtain satisfactory sexual performance.1
Erectile dysfunction may have a significant impact on relation- ships with a partner and family. One of the problems that men with erectile dysfunction experience is shame and discomfort associated with the discussion of the condition. This discourages these men from seeking consultation from their physicians and vice versa. There was no easy and effective treatment for erectile dysfunction in the past. However, in recent years there has been a significant advancement in the knowledge concerning the physiology of erection allowing the mechanisms of penile erection to be better understood. These advancements have allowed research in erectile dysfunction management to gain significant development.
An epidemiological study carried out by The Massachusetts Male Aging Study (MMAS) between 1987 and 1989 revealed the prevalence of erectile dysfunction in US male population to be as high as 30 million.2 The highest prevalence was found in men aged between 40 and 70 years old at 52%, with 17%, 25%, and 10% corresponding to mild, moderate, and severe degree of dysfunction respectively. Mild degree of dysfunction refers to the condition where penis erection can be achieved long enough for completion of sexual intercourse but not always. Moderate degree of dysfunction refers to the condition where penile erection can only be achieved and maintained for completion of sexual intercourse some- times. Severe degree of dysfunction refers to the condition where penile erection cannot be achieved and maintained for completion of any sexual intercourse.
A Thailand Erectile Dysfunction Epidemiology Study (TEDES) examined the prevalence of erectile dysfunc- tion in 1,250 Thai men aged between 40 and 70 years in 1998 and found the prevalence of mild, moderate, and severe degree of erectile dysfunction to be 19.1%, 13.7%, and 4.7% respectively.3 The overall prevalence estimation from the TEDES study was 37.5% (Figure 1).
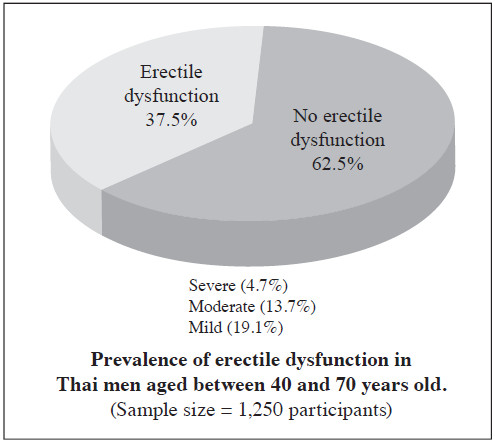
Figure 1: Prevalence of erectile dysfunction (ED) in Thai men.
Penile erection is achieved when the emissary venous drainage is impeded due to compression of tunica albu- ginea caused by an increased in blood flow to the penis due to sexual stimulation. In recent years, the neurotrans- mitter critical for achieving an erection was determined to be nitric oxide, previously known as endothelium-derived relaxing factor (EDRF).4,5 This finding has led to wide- spread development of treatments for erectile dysfunction.
1.Anatomy of penis
The penis contains three cylindrical erectile tissues; two corpus cavernosa and one corpus spongiosum containing the urethra.6 The corpus cavernosum is surrounded by a thick and tough layer of tunica albuginea. The intercavernous midline septum that separates the two corpus carvernosum contains many tiny spaces on the ventromedial side of tunica albuginea that may be perforated easily during penile implant surgical procedure. The inside of copus cavernosum is filled with sinusoidal tissue surrounded by a vascular endothelium layer called trabeculae. The two corpus cavernosa lie parallel to each other and separate at the bulb of penis forming the crus of the penis that attaches to the pubic arch.
2.Anatomy of blood vessels
The artery that provides blood supply to the penis is called the internal pudendal artery that branches from the internal iliac artery. The distal portion of the pudendal artery forms the common penile artery that branches into dorsal, bulbourethral, and carvernous arteries. The carvernous arteries further branch into helicine arterioles with convoluted appearance draining into the sinusoidal tissue of the penis.
The blood inside the corpus cavernosa is drained into the emissary veins via tiny subtunica venules perforating the two layers of tunica albuginea. An erection is achieved when the sinusoidal tissue of the penis is filled with blood from the arterial supply causing the tissue to become swollen. The erection causes the tunica albuginea layer to become distended resulting in the mechanical compres- sion of subtunica venules between the layers of tunica albuginea that subsequently lower or prevent blood drainage from the penis.
3.Anatomy of nerve supply
The peripheral nervous system responsible for sensory and erection control can be divided into two groups, namely autonomic nervous system and somatic nervous system. Penile erection is regulated mainly by the para- sympathetic branch of the autonomic nervous system that contains the control center located at S2-4 known as the sacral erection center. The nerves that exit the center and form a preganglionic plexus are called the pelvic nerve or nervi erigentes (Figure 2).
The sympathetic branch of autonomic nervous system exits the spinal nerves at T10-L2 level. The preganglionic fibers join together to form the sympathetic chain (Figure 2) that connects with the inferior mesenteric plexus and superior hypogastric plexus. The preganglionic fibers from the pelvic nerve will join with the postganglionic fibers from the superior hypogastric plexus forming the pelvic plexus that gives rise to the cavernous nerve that regulates penile erection.
The somatic nervous system exits the spinal nerves at level S2-4 and innervates the penis via the pudendal nerve. The nerve contains both sensory and motor neurons. The motor efferent fibers innervate the ischiocarvernosus and bulbocarvernosus muscles and terminate at the dorsal nerve of the penis. The distal end of the dorsal nerve of the penis fans out and is responsible for carrying the sensa- tion from the skin around the perineum, glans penis, and tunica albuginea.
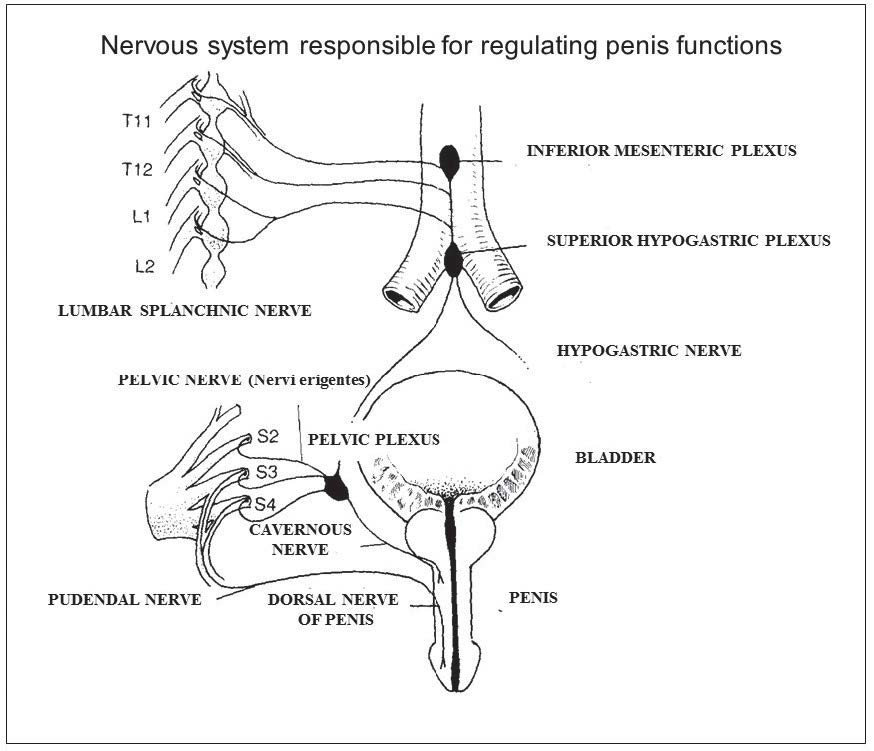
Figure 2: Peripheral nervous system responsible for controlling penile erection.
4.Mechanisms of penile erection
The mechanisms involved in penile erection can be divided into three types.
a)Nocturnal erection: A normal male experiences 3-5 nocturnal erections per night each lasting around 30-40 minutes.7 Nocturnal erections occur during rapid eye movement (REM) sleep. It is still unclear how and why nocturnal erection happens.
b)Psychogenic erection: The brain is responsible for regulating erection following sexual stimulation (Figure 3). It is still unclear what parts of the brain are involved in controlling this response. The signal travels through the medial preoptic area (MPOA) near the anterior hypothalamus before going to the sacral erection center via lateral funiculus of the spinal cord.8
c)Reflexogenic erection: Reflex erection of the penis occurs when the signal from direct stimulation of the penis travels past the dorsal nerve of the penis to the sacral erection center. The motor pathway travels to the penis from the sacral erection center through pelvic nerve, pelvic plexus, and cavernous nerve respectively.
5.Neurotransmitters and chemicals
5.1 Central neurotransmitters
A number of neurotransmitters are involved in regulating penile erection including prolactin, opioids, and oxytocin. Studies have shown that dopaminergic stimulation causes sexual arousal and erection. It is believed that stimulation of the D2-like dopamine receptor located at the paraven-tricular area causes oxytocin production.9 Oxytocin has been shown to be released during sexual intercourse and injection of oxytocin to the paraventricular area in mice induced sleepiness and penile erection.10, 11 The mechanism of how oxytocin function in erection remains unclear but it is believed to be involved with release of nitric oxide (NO).
5.2 Peripheral neurotransmitters
Stimulation of the sacral erection center from either psychogenic or reflexogenic origins will cause the nerve impulse to travel through the cavernous nerve via cholinergic neurons releasing acetylcholine (Ach) and vasoactive intestinal peptides (VIP) (Figure 4). The end of the cavernous nerve also contains axon terminals from another type of neuron that releases nitric oxide, the most important neurotransmitter in regulating penile erection. These neurons are called nonadrenergic-noncholinergic neurons (NANC). Therefore there are two pathways that cause erection of the penis following stimulation: the nitrergic pathway that releases nitric oxide; and the vipergic pathway that releases Ach and VIP.
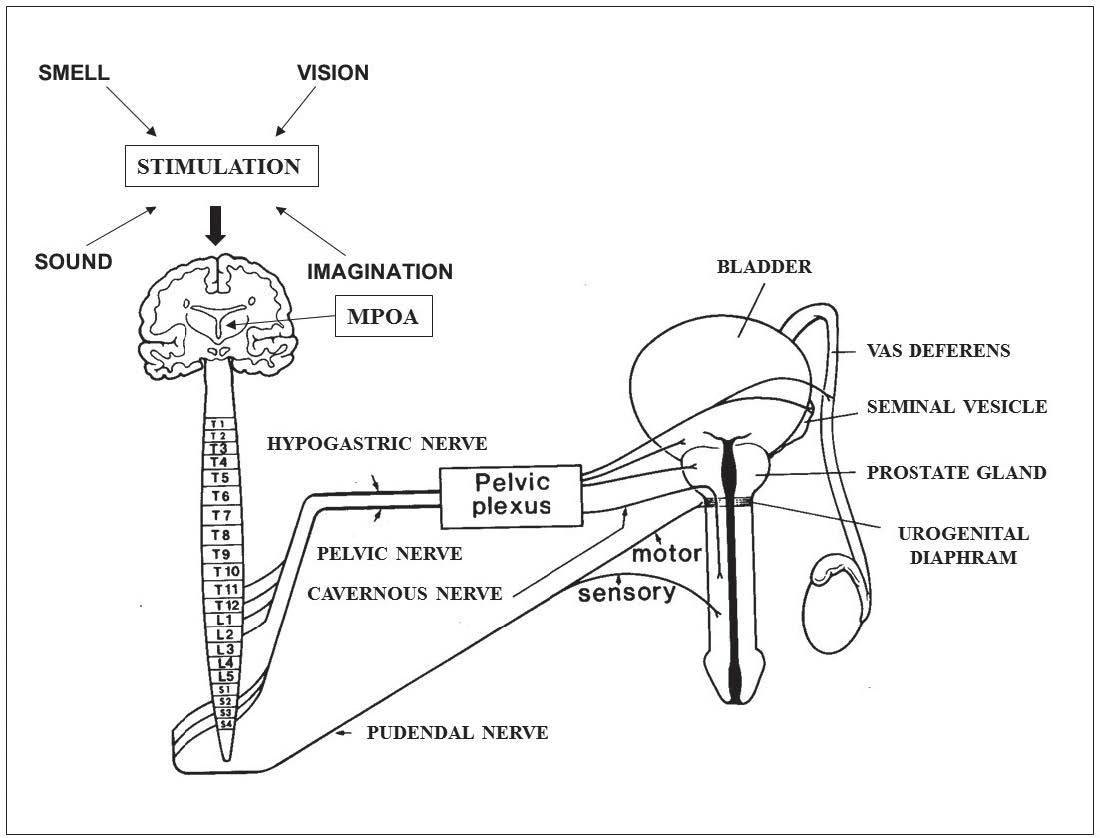 Figure 3: Mechanisms of psychogenic erection via medial preoptic area (MPOA) and reflexogenic erection via pudendal nerve are shown in this figure.
Figure 3: Mechanisms of psychogenic erection via medial preoptic area (MPOA) and reflexogenic erection via pudendal nerve are shown in this figure.
Nitric oxide activates guanylate cyclase that catalyzes the production of cyclic guanosine monophosphate (cGMP)13-16 and induces protein kinase G causing a reduction in intracellular calcium levels. Meanwhile the binding of VIP to receptors on the cavernous smooth muscle cell membrane causes activation of the G protein- coupled receptor leading to cAMP production through the activity of adenylate cyclase. cAMP functions as a secondary messenger capable of activating protein kinase A and this can also cause the intracellular calcium level to decline. The decrease in the calcium level causes trabecular smooth muscle relaxation. The gap junctions between the cavernous smooth muscle cells contain a pro- tein called connexin 43, 0.25 micron in size. The presence of these gap junctions helps the muscular cells to contract and relax together,17 allowing erection to be achieved.
cGMP is broken down by phosphodiesterase type 5 (PDE 5) enzyme into guanosine monophosphate (GMP) which is inactive. PDE 5 inhibitors, such as sildenafil, can be used to treat erectile dysfunction. Similarly, cAMP is broken down by phosphodiesterase type 2 and type 3 (PDE 2, 3) enzymes into inactive adenosine monophos- phate. Other PDE enzymes can be found in other organs such as the brain, cardiac muscle, vascular smooth muscle, adrenal gland, platelet, and retina.18 There are about 11 PDE isoenzymes that have been identified.48
Research conducted by Goldstein and members, a study of 861 patients with erectile dysfunction, suggested that the causes of the disorder are from organic, psychogenic, or from both origins (mixed ED) with the prevalence per- centages of 70%, 11%, and 18% respectively.
The factors causing erectile dysfunction can be classified as follows:
1. Arterial disorder
The primary cause of erectile dysfunction, responsible for 60-80% of the cases,20 is atherosclerosis resulting from various factors such as hypertension, hyperlipidemia, diabetes mellitus, radiotherapy, and changes associated with aging. Treatment of erectile dysfunction due to arterial disorder by blood vessel surgical procedures cannot always be carried out because the patients are often elderly with chronic diseases. Localized obstructive arterial abnormalities that can be treated with a surgery are found in patients who are young and the conditions have resulted from an accident.
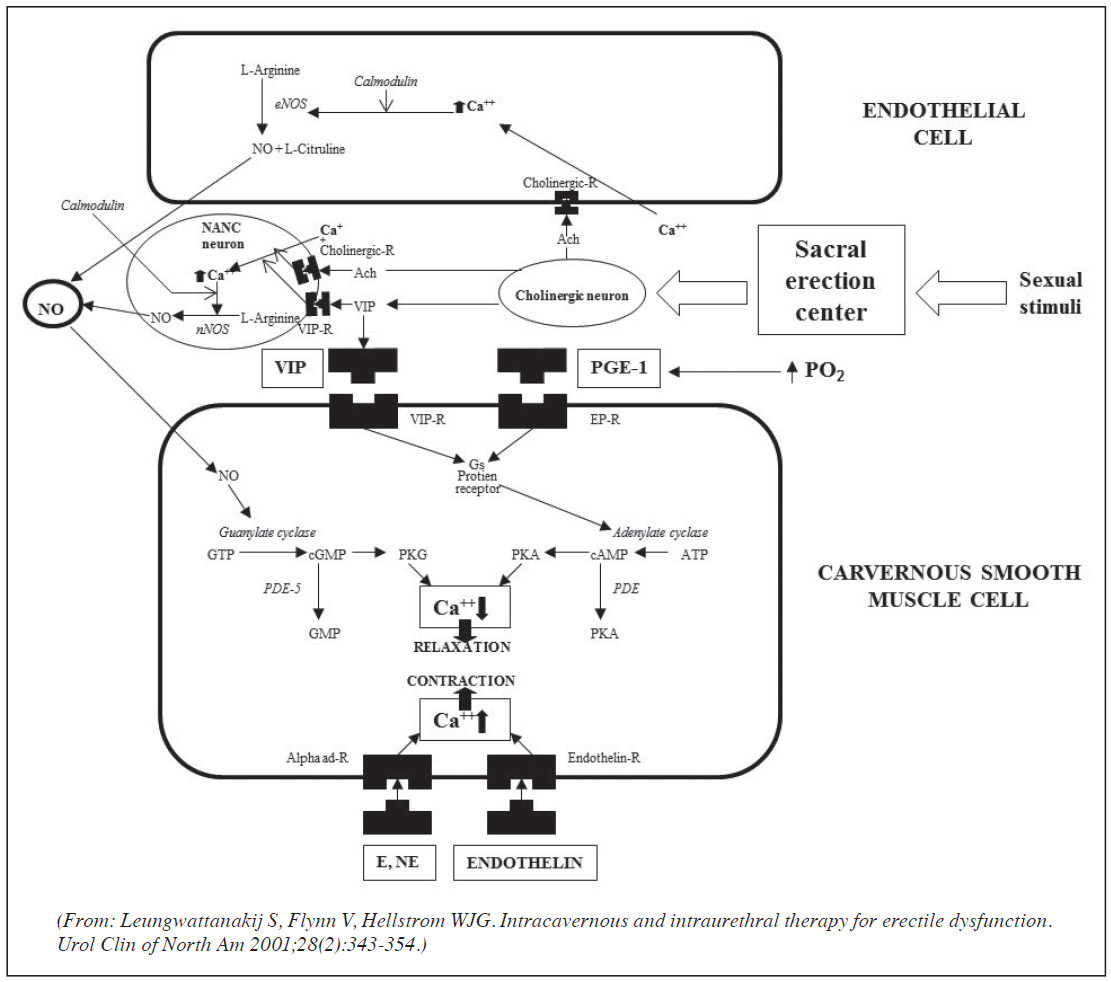 Figure 4: The pathways involved in causing a penile erection after stimulation. The nitrergic pathway uses nitric oxide that induces the production of cGMP and the vipergic pathway uses Ach and VIP that stimulate the production of cAMP. Both cGMP and cAMP cause a reduction in intracellular calcium level that causes relaxation of the smooth muscle.12
Figure 4: The pathways involved in causing a penile erection after stimulation. The nitrergic pathway uses nitric oxide that induces the production of cGMP and the vipergic pathway uses Ach and VIP that stimulate the production of cAMP. Both cGMP and cAMP cause a reduction in intracellular calcium level that causes relaxation of the smooth muscle.12
[GTP (guanosine triphosphate), cGMP (cyclic guanosine monophosphate), GMP (guanosine monophosphate), ATP (adenosine triphosphate), cAMP (cyclic adenosine monophosphate), AMP (adenosine monophosphate), PKG (protein kinase G), PKA (protein kinase A), Vasoactive intestinal peptide (VIP), VIP-R (VIP receptor), EP-R (prostaglandin receptor), eNOS (endothelial nitric oxide synthase), nNOS (neural nitric oxide synthase), NANC (nonadrenergic noncholinergic), PDE (phosphodiesterase), Ach (acetylcholine), E (epinephrine), NE (norepinephrine), Alpha ad – R (alpha adrenergic receptor), NO (nitric oxide)].
2.Venous and sinusoidal disorder
Erectile dysfunction with impaired veno-occlusive function of the penis may be caused by fibrosis in the corpus cavernosum due to prolonged penile erection or Peyronie’s disease. Castration in mice have resulted in fibrosis of the corpus cavernosum and venous leakage.21
3.Neurogenic disorder
Erectile dysfunction due to neurological causes can be divided into those caused by disorders of the brain, such as brain tumor, epilepsy, cerebro vascular accidents (CVA), Parkinson’s disease, and Alzheimer’s disease, and those from disorders of the spinal cord, with the most common cause being spinal cordinjuries that affect the afferent and efferent nerve pathways or both. Disorders of the peri- pheral nervous system including the cavernous nerve of the autonomic branch and pudendal nerve of the somatic branch can also cause erectile dysfunction. The most common condition of peripheral neuropathy found by general practitioners is diabetes mellitus since the disease can cause damage to both vascular and nervous systems. Diabetes mellitus is responsible for 30% of erectile dysfunction.22
4.Hormonal disorder
Diseases of the endocrine system that may decrease sexual desire include hypogonadism, hyperthyroidism, Cushing’s syndrome, Addison’s disease, and hyperprolactinemia.
5.Psychological disorder
Psychological processes that can cause erectile dys- function are depression and fear of sexual intercourse commonly seen in men with obsessive and compulsive disorder and anxiety. Other psycho logical factors may be the results from other illnesses or conditions, such as men who suffer from premature ejaculation may experience erectile dysfunction because they constantly fear and worry that they will ejaculate prematurely again.
6.Other risk factors
There are a number of other risk factors that can contribute to erectile dysfunction especially many types of medications.
1. Patient history
In practice, a number of patients often consult their physicians concerning erectile dysfunction symptoms unaware that they also have diabetes mellitus or hyper- tension. While obtaining the patient medical history, it is important to also ask about the sexual history in detail. Moreover, information concerning the socioeconomic status of the patient should be obtained. Given that the treatment plan for each patient is unique and must be suitable for that particular patient, the doctor may order additional specific diagnostic studies using the patient goal-direct approach. For example, patients who choose to treat their erectile dysfunction with oral medications or vacuum erection devices should be diagnosed with standard procedures. Patients who have chosen to undergo more invasive surgical options should receive diagnostic tests, such as rigiscan and ultrasonography, to confirm the causes of the condition to be truly organic.
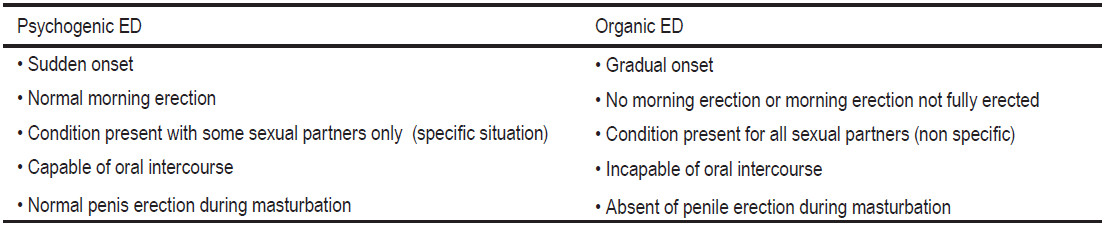
The detailed sexual history of the patient can be used to help distinguish erectile dysfunction from other sexual problems. General practitioners have found a large number of patients who misunderstood their premature ejaculation problem for erectile dysfunction. Assessment of the patient’s psychological problems and relationships with patient sexual partner can help distinguish whether the erectile dysfunction is psychogenic or organic as shown in Table 1. The physician should inquire about existing medical conditions and explain information concerning the limitations and risks of each erectile dysfunction treatment with the patient. Formalized sexual question- naires, such as the International Index of Erectile Function (IIEF) especially an abbreviated 5-item version called Sexual Health Inventory for Men (IIEF-5), can be com- pleted easily by the patient. However, some physicians believe that this method is suitable for research purposes only because the score before and after treatment can be compared.
Table 1: Characteristics listed in this table can be used to help distinguish psychogenic erectile dysfunction from organic erectile dysfunction.
2.Physical examination
Beside the normal physical examination of erectile dysfunction patients, it is beneficial to assess the blood pressure and pulsation of the limbs, the lower limbs in particular. The presence of bruit may indicate underly- ing vascular conditions such as an aneurysm. Secondary sexual characteristics examination for hair distribution, gynecomastia, and testicular consistency and size can also be done.
Neurological examinations measure the motor and sensory function of the lower extremities. Evaluation of the cremasteric reflex (L1-2) can be done by assessing the activity of the anal sphincter muscle upon stimulation of glans penis. This evaluation is recommended for patients who are older than 50 years old. Examination of the prostate gland can be carried out while testing for the cremasteric reflex. Palpation of the penis can be done to detect the presence of fibrous plaque or curvature of the penis in Peyronie’s disease. All of these causes for erectile dysfunction should be treated simultaneously.
3. Laboratory examinatio
3.1 Standard laboratory examinations
The following standard laboratory analysis must be done in all erectile dysfunction patients, regardless of the cause: complete blood count, urinalysis, fasting blood sugar, lipid profile, renal function test, and liver function test. Diabetes mellitus and hyperlipidemia have been identified as important conditions that can cause erectile dysfunction.
3.2 Endocrine evaluation of testosterone and prolactin
A study carried out by Buvat and team23 revealed that the measurement of serum testosterone levels should be done for patients who are younger than 50 years old and have experienced loss of libido or testicular abnormalities, since a low serum testosterone level was only found in 4% of patients. For patients aged over 50 years, analysis of serum testosterone level is recommended for all patients because a low serum testosterone level was found in 9% of the patients. The measurement of prolactin level is only recommended in patients with loss of libido, gynecomastia, and/or testosterone levels below 400 ng/dl (4 ng/ml) since the condition of prolactinoma was found only in 1 out of 1,022 individuals.
3.3 Examination for risks for ischemic heart disease
The dangers posed by ischemic heart disease during sexual activity do not come from any known medications for treating erectile dysfunction. Instead these dangers are directly related to the sexual activity itself because sexual intercourse demands a relatively fit condition. A large number of patients with erectile dysfunction are elderly who have not engaged in any sexual activity for a long period of time. Therefore it is important for the physician who will prescribe medications for the treatment of erectile dysfunction to take the risk of ischemic heart condition into account.
3.4 Additional special examination
3.4 .1 Nocturnal erection examination
Examination for the presence of nocturnal erection may help confirm the psychogenic cause for erectile dys-function. This evaluation is very important for patients who will undergo surgical procedures, especially penile prosthesis implantation, to treat their erectile dysfunction condition. Rigiscan is a widely used tool that can continu- ously measure the frequency, size, and rigidity of erection throughout the night.24 Normal males will have at least one nocturnal erection with an increase in the diameter of the penis base exceeding 3 cm and the tip exceeding 2 cm, the rigidity of the penis must be above 70% compared with flaccid penis, and last for at least 10 minutes.25 The average number of nocturnal erections is 4-5 times per night lasting over 30 minutes in total.26
3.4 .2 Penile blood vessel examination
Examination of the blood vessels in the penis can be done using a duplex Doppler ultrasound device with an injection of vasoactive agents that can point out causes of erectile dysfunction due to abnormalities of penile arterial and venous blood vessels. The procedure can also be used as a screening test before more invasive tests, such as pudendal angiography or cavernosometry and caver- nosography, are performed. Utilization of color imaging technique has been incorporated into the procedure (color Doppler ultra-sonography (CCDU)), and this allows faster detection of small cavernous arteries.27 A number of institutes also recommend simultaneous stimulation of the penis or utilization of audiovisual sexual stimulation (AVSS).28 This procedure may cause patients to feel anxious, therefore the results can only be used to determine whether the cause of the erectile dysfunction may be due to the conditions related to the arteries and veins in the penis. For patients who have to undergo vascular surgeries, a pudendal angiography must be carried out for patients with arterial insufficiency and cavernosometry and phar- macocavernosography in patients with veno-occlusive dysfunction.
3.4 .3 Examination of the nervous system regulating penile erection
Examination of the nervous system responsible for erection regulation as a diagnostic tool is not widely used since erectile dysfunction with a sole neurological cause accounts for about 10% of cases.29 The majority of cases are associated with diabetes mellitus and occur after radical surgery indicating that the condition is caused by multiples factors involving vascular conditions and other psychological entities. More importantly, the determination of erectile dysfunction due to neurological origins is often obtained from assessing the patient’s medical history and a neurological examination.
The patient’s sexual partner should also be brought in to visit the doctor where possible since it may improve the outcome of the treatment. A positive relationship between the physician and patient can be strengthened by educat- ing the patient about the condition. The doctor should also provide other recommendations to promote healthy behaviors, such as exercising regularly, avoiding or min- imizing risks that may worsen the condition or impede treatment success, including hyperlipidemia, hyperten-sion, hyperglycemia, smoking, alcohol consumption, and usage of certain medications.
Psychotherapy and sex therapy were widely used in the past to treat erectile dysfunction, but were expensive, required long treatment periods, and had a high chance of reoccurrence. It is now known that a large number of cases of erectile dysfunction are due to organic causes. Treatments that are easy and convenient to use include oral and intraurethral drugs. In principle, the treatment of erectile dysfunction should start from easy to hard, taking into consideration convenience, cost, and ease of usage. It is important for the physician to always take the patient and his partner psychological conditions into account when choosing an appropriate treatment. Patients who are struggling with his partner or at work should be advised to seek attention from a psychiatrist.
1. Treatment with oral medications
1.1 Phosphodiesterase type 5 (PDE 5) inhibitors
The class of medication functions by inhibiting the activity of PDE 5 enzyme that is responsible for degrada- tion of cyclic guanosine monophosphate (cGMP) in corpus cavernosum and relaxation of smooth muscle around the sinusoids (Figure 5). As a result, there is an increased volume of blood inside the penis leading to the develop- ment of an erection. PDE 5 inhibitors do not directly cause the relaxation of the smooth muscle, therefore an erection cannot be achieved without the activities of nitric oxide and cGMP, both of which are produced in response to sexual stimulation. In other words, the medication can help prolong an erection after sexual stimulation. Sildenafil (Viagra™) was the first drug of this class and is widely used. The drug is available in three doses, 25mg, 50 mg, and 100 mg. The starting dose should be 50 mg, except for patients with liver diseases, kidney failure or aged 65 or older where the starting dose should be adjusted to 25 mg per day. The dose can be increased to 100 mg where the desired effect is not yet obtained and the adverse effects are absent. However, if the patient is responsive but experiences adverse effects, the dose can be lowered to 25 mg. In general, a better response is obtained with a higher dose but adverse events are more common. Around 75% of patients show response to a 50mg dosage. The dose that was seen with second highest response rate was 100 mg. Sildenafil should be taken 1 hour prior to sexual activity because the highest level of the drug inside the blood is seen within 30-120 minutes (average 60 minutes). In practice, the effects of the medication can be seen as early as 30 minutes in some patients, where normal sexual arousal can promote an erection and the medication help sustains it. The drug should be taken while the stomach is empty. When sildenafil is taken with food, especially with high amount of fats, the absorption time is increased thereby lowering the level of the drug in the blood around 29% at 60 minutes time point. The half-life of sildenafil is approximately 4-5 hours, therefore some patients have reported to be able to complete sexual intercourse after waking up in the morning despite have taken the drug before going to sleep.
The results from Asian Sildenafil Efficacy and Safety Study (ASSESS), that examined the effects of sildenafil in Asian men including Thailand, found an improvement in erectile function of 81.0-88.5% in the group treated with the drug compared with 28-38% in the placebo group. A significantly higher percentage of the subjects that were able to complete sexual intercourse were found around 67.8-74.0% in the treatment group compared to 27.0-30.5% from the placebo group. A study that evaluated the safety of sildenafil in a large number of samples by comparing the data with the placebo group for 1 year,31 reported the adverse effects as summarized in Table 2. Most of the adverse side effects were temporary and mild. The pres- ence of these effects can be explained by the mechanism of the drug, for example, vasodilation can also occur in blood vessels inside the brain causing headache. General vasodilation of blood vessels around the facial and nasal regions may cause the subject to experience flushing and nasal congestion. Relaxation of the smooth muscle surrounding the gastrointestinal tract may cause dyspepsia. Abnormal vision, with blurry images, impaired ability to distinguish green and blue colors, and addition of blue color into vision, may be explained by the fact that silde- nafil can also inhibit the activity of PDE 6, an enzyme involved in phototransduction inside the retina.30
Sildenafil must not be taken with any nitrate medications. Nitrates can significantly increase the level of nitric oxide and cGMP in the blood, therefore when they are taken with sildenafil, a lethal hypotension condition may ensue. Taking sildenafil with hypertensive medications does not have any significant synergistic effects. When sildenafil is taken with cimetidine, ketoconazole, and erythromycin, the level of sildenafil is abnormally high because these medications inhibit the activity of cytochrome P3A4 in the liver, which inhibits the activity of sildenafil.
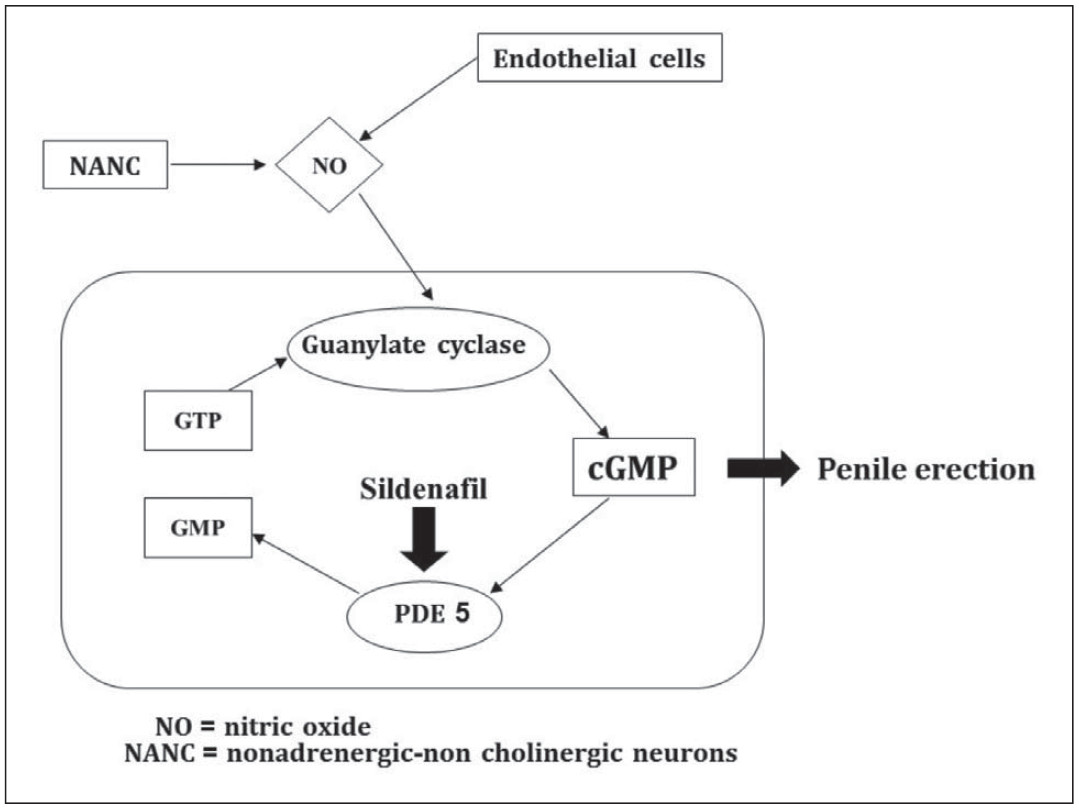 Figure 5: Mechanisms of sildenafil.
Figure 5: Mechanisms of sildenafil.
Table 2: Adverse effects from sildenafil compared with placebo.
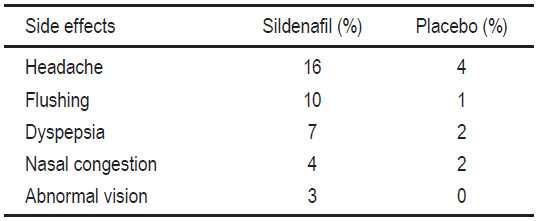
Table 3: Inhibitory concentrations of sildenafil, tadalafil, and vardenafil
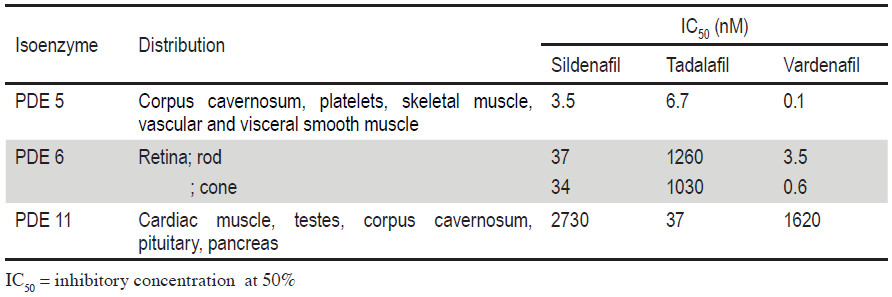
Other PDE 5 inhibitors that can be taken orally32 are Cialis™ (tadalafil or IC351) by Lily-ICOS and Levitra™ (vardenafil or BAY 38-9456) by Bayer-GSK. The advan- tages of tadalafil are that there are no restrictions on the type of food that can be consumed, no abnormal vision because the 50% inhibitory concentration (IC50) of PDE 6 is significantly higher than PDE 5 (Table 3).48,49 The half- life of tadalafil is 17.5 hours which is significantly longer than sildenafil. However, the IC50 of tadalafil is only 5.5 times higher against PDE 11, an enzyme found in high amount inside the cardiac muscle, compared with PDE 5. Although the exact functions of PDE 11 inside the cardiac muscles are still unclear, there are no adverse effects on the heart in phase III study and tadalafil is considered to be very safe. It is worth looking out for other adverse ef- fects in the future when tadalafil goes to the market and is widely used. Vardenafil has a pharmacokinetic profile very similar to that of sildenafil, with a slightly shorter time for peak blood level. The half-life of vardenafil is 4-5 hours. There is also no restriction on taking the medica- tion with any food. The efficacy and side effects of these three drugs are very similar.
Low dosage of tadalafil of 5 mg/ml has been used as a treatment for patients who have frequent sexual activities. Studies have indicated that daily administration of the drugs at 5, 10, and 20 mg yielded similar efficacy but the 5 mg dose had the lowest adverse effects,51-52 and lower adverse effects compared with taking the drug on demand with 10-20 mg dose. Treatment daily with 2.5 mg/day had a higher response compared with placebo but the efficacy was lower than 5 mg dosage.
It was later reported that daily treatment of a low dose of tadalafil can help treat patients with lower urinary tract symptoms (LUTS). The recommended dosages were 2.5 and 5 mg/day, with 5 mg dose giving better response com- pared with 2.5 mg, but no significant differences when compared with 10 mg and 20 mg doses similar to findings from the erectile dysfunction study.53
There are three additional PDE 5 inhibitors that are available on the market but are not being sold in Thailand. This is because after the expiration of sildenafil patent, other brands have been sold at lower prices, especially Sidegra that is manufactured by Thailand’s Government Pharmaceutical Organization (GPO), making it less prof- itable for sale in the Thai market. These three drugs are Avanafi (Stendra), Udenafil (Zydena) and Mirodenafil (Mvix) with similar efficacy profiles compared with older PDE 5 inhibitors but with different half-life and adverse effects.54-56
1.2 Medications with a central acting mechanism
Apomorphine is a D2-like dopamine receptor antagonist distributed by Abbott Laboratories (Uprima™) and Takeda (Ixense™) in Thailand. It is the first medication that was used to treat erectile dysfunction with its effects on the central nervous system or directly at the hypothalamus (paraventricular nucleus). The medication is taken orally by placing the drug under the tongue to allow fast absorption. The effects can be seen within 10-25 minutes. The doses that were used in studies ranged from 2-6mg but most research used a dose ranging from 2-4mg. The results showed that completion of sexual activity were seen in 41.5% and 50.6% of the subjects who received 2 and 4 mg doses respectively. Only a few mild adverse effects, that corresponded to the dosage, were reported with the most common being nausea that was found in 2-8% of the subjects. The efficacy of the drug at 3 mg. dose is very similar to that of 4 mg. but with lower risks of adverse effects, so only 2 and 3 mg dose are available on the market. The main benefit of this drug class is that it can be taken with nitrate medications. However, the drug cannot be used to treat erectile dysfunction caused by spinal cord injuries and nerve damage. This drug is no longer sold in Thailand.
1.3 Other oral therapies
Another erectile dysfunction medication that used to be popular in the past was trazodone,30 an anti-depres-sive drug that works by inhibiting serotonin reuptake along with peripheral α2-adrenoceptor blocking activity. The efficacy profile of trazodone was not very high with adverse effects of headache, nausea, sleepiness commonly reported. Trazodone should only be used to treat psycho- genic erectile dysfunction.
2. Intraurethral medications
The intraurethral medication for treating erectile dysfunction is called intraurethral alprostadil or MUSE™ (Medicated Urethral System for Erection) distributed by Vivus (Menlo Park, California) with doses of 125, 250, 500, and 1,000 micrograms. The medication is to be inserted through the urethra before sexual intercourse (Figure 6). The license of this medication in Thailand belongs to Abbott.
Alprostadil that has been administered via the urethra will be absorbed into corpus cavernosal tissue via communicating vessels that link the corpus spongiosum and corpus cavernosum.12 After the drug is inserted in the urethra, it will take approximately 8 minutes for the effects to be seen with full erection achieved after 20 minutes. The effects of the medication will wear off after about 60 minutes.

Figure 6: MUSE™ applicator stem is inserted into the urethra often after urination to provide moisture. The button is gently pressed to deposit the pellet inside the urethra. Massage the penis with both hands to dissipate the drug and help speed up absorption.
Hellstrom and team found that treatment with MUSE™ at 500 micrograms dosage yielded satisfactory penis erection in 26.7-39.6% and slightly higher percentages of 31.7-48.8% for 1,000 micrograms dosage.34 Lower dosages at 125 and 250 micrograms do not provide a satisfactory level of erection. Therefore, the starting dose for MUSE™ should be 500 micrograms and a higher dose of 1,000 micrograms can be increased where the patients are not yet satisfied with the lower dose.
The most common adverse effect of MUSE™ is urethral burning pain that is experienced in 10-30% of the cases. Other side effects that are found in small numbers include infection of the urethra and priapism.35 Patients who are at risks of priapism, have penis curvature, and are allergic to alprostadil should not use MUSE™.
A study examining the effects of transurethral PGE1 with prazosin showed a slightly higher response than PGE1 alone.36 Other medications, including nitric oxide donors, given intraurethrally did not provide a better response than those that were taken orally.37
3. Intracavernosal injection therapy
The most common starting intracavernosal injection drug is alprostadil. Other medications include papaverine, a non-specific PDE 5 inhibitor, and phentolamine, an alpha adrenergic antagonist, are often used as a second-line injection drugs and are mixed with alprostadil36 called tri-mixed therapy.12
The injection drug that is currently under research is forskolin which promotes direct adenylate cyclase activa- tion that increases the level of cyclic AMP (Figure 4) and is injected with Invicrop™ (vasoactive intestinal peptide + phentolamine).36 Other medications that can be given when standard intracavernosal injections are irresponsive are potassium channel openers which function through the potassium channel causing muscle relaxation similar to calcium channel drugs.
The efficacy of this method is around 90% with pro- longed erection (erection exceeding 4 hours) as the main side effect found in 1-6.9% of the subjects, with the highest being papaverine and lowest being PGE1. Long-term usage may cause fibrosis which has been reported in 4.1- 5% of cases.35
Intracavernosal injection therapy is unpopular since patients not only have to learn how to correctly perform the injection but also are afraid of performing injection into their own penises. The medication can also cause pro- long pain especially in PGE1 drugs due to lowering of the pain threshold receptor or the pH of the medication itself remains unclear.12
4. Vacuum devices
A vacuum constriction device (VCD) works by using the vacuum pump to increase the blood flow into the penis and application of a constrictor ring to retain the blood and remain erect. The device contains three pieces of equipment; a cylinder, a vacuum pump, and a constrictor ring (Figure 7). The pump may be manually operated by pumping action of the hand or used a battery-operated automatic vacuum pump. Certain pump models contain a built-in valve that automatically opens when the pressure inside the chamber falls below the safety level and to ensure that the pump does not exceed 250-350 mmHg.38
Vacuum constriction devices should not be used in patients who have bleeding disorders, are taking antico- agulants, or have a history of priapism. However, the utili- zation of vacuum constriction devices in patients who are taking anticoagulants has also been reported to be safe. Some men with Peyronie’s disease cannot use the device because the curvature of the penis may cause pain if the penis is inserted into a small and straight cylinder.
5. Penile prosthetic devices
There are many types of penile prostheses. For ease of understanding, the penile prostheses will be classified into two classes, nonhydraulic and hydraulic penile prosthesis. Each class can be further divided according to the appear- ance of the prosthetic shaft.39
5.1 Nonhydraulic penile prostheses
Nonhydraulic penile prosthetic devices have simple mechanics therefore have lower risk of mechanical failures.The disadvantages of these devices are abnormal feel and appearance, hard to conceal, and the size of the enlargement cannot be controlled.
 Figure 7: A vacuum constriction device.
Figure 7: A vacuum constriction device.
5.2 Hydraulic penile prostheses
Hydraulic penile prosthetic devices allow fluid to be pumped from the reservoir into the penis shaft to obtain an erection. The fluid can be returned to the reservoir to allow the penis to return to the flaccid state (Figure 8). This type of device permits better concealment and allows enlarge- ment during erection. Newer generations of these devices can also provide penis enlargement of the length during an erection. The devices can be easily inserted through a small surgical opening of the penoscrotal junction (Figure 9). The hydraulic penile prostheses can be further categorized according to the number of equipment. Newer pumps are larger and can easily be deflated with one press of a button (AMS 700 momentary squeeze or MS pump).57
Patients who should be treated with penile prostheses are those with organic erectile dysfunction who are not responding to other treatments. For those who have psychogenic erectile dysfunction, penile implants should only be performed when other treatments have failed and advice from psychiatrists regarding the surgical procedure should be provided. Most of the procedures carried out today use the hydraulic penile devices because they offer a more normal look and feel. The advantages and disadvantages of each device should be thoroughly explained to patients. It is important to take the limitation of dexterity in some patients into consideration, since it may be difficult to operate the pump and return the fluid to the reservoir. Patient’s partners should also be educated about the device and be ask whether they can help assist the patients with device operation.
Despite high satisfaction above 90% and low risks of complications from the surgical procedure, the high cost of the device causes some minor complications to become more severe. The physician must try to minimize the risks of complications. Some of the complications are discussed here.
a) Corporal crossover: The distal part of the corpus cavernosum septum is very fragile and can easily be perforated. The perforation in the medial septum side may be minimized by positioning the dilator in the center to the lateral side.
b) Corporal perforation: Perforation across tunica albuginea may occur at proximal and distal corpus cavernosa and urethra, but is more frequently observed with the proximal corpus cavernosa. This condition is commonly found in patients with fibrosis with unknown cause or those with Peyronie’s disease.
c) Perforation of the urethra: This complication is rare but can be severe and usually occurs at the end of the urethra.
d) Perforation of penile implant: Erosion and extrusion of the penile prostheses usually happens with an infection. Patients with compromised tissues, such as those with diabetes mellitus or patients who have preexisting infections from previous penile implants, are more susceptible. This complication is more common in the semi-rigid rod type which is no longer used.
e) Glans bowing (SST deformity): Deformity of the glans penis formed during erection that may cause pain during erection and sexual intercourse.
f) Infection: Although infections caused by penile implants are rare, the condition may be very dangerous. A prevalence of infection with the penile implant of 0.6-3.0% has been reported in the rod prosthesis group and 0.8-8.9% in the multicomponent inflatable prosthesis group.40 Staphylococcus epidermidis is the most common cause of infection. This type of bacteria can normally be found on the skin surface. Risk of infection is higher in patients with diabetes mellitus, impaired spinal cord, who are immune-deficient, and have or frequently use a catheter. Some companies now coat a layer of antimicrobial substance that can minimize colonization of bacteria.50
g) Mechanical malfunction: Newer models of three-piece prostheses have an incidence of malfunction lower than 5%. Most failures involve leakage at the junction between the pumps and the cylinders, bending of the tubing, and problems at junctions.
h) Autoinflation: This happens when the device is inflated without the pumping action

Figure 8: Three-piece hydraulic penile implant- consisting of the cylinders, pump, and a reservoir bag.

Figure 9: A surgical procedure installing a three-piece penile implant at Bangkok Hospital through a small incision at the penoscrotal junction.
6. Vascular surgery
Vascular surgery is not practiced widely despite the fact that abnormalities of penile blood vessels are important causes for erectile dysfunction. A long period of treat- ment and a low success rate has made vascular surgery an unpopular method of treatment. This procedure is only carried out when a specific pathology of the vascular system has been identified, for instance a young male who has erectile dysfunction after an accident causing damage to pelvic blood vessels. Ligation of venous vessels are sometimes carried out in patients whose arteries are still functioning normally from the test using duplex Doppler ultrasound and have confirmed venous leakage from cavernosography despite high chance of reoccurrence.
7. Combination therapy
Utilization of multiple medications with different properties to simultaneously treat erectile dysfunction has been gaining a lot of attention in recent years. For example, treatment with MUSE™ and sildenafil in 16 patients with suboptimal response to monotherapy provided satisfactory outcomes for 3 months evaluation period.41 A similar study showed that 60 of 65 patients reported satisfactory response using IIEF score assessment.42 Another study using 4 mg of doxazosin given orally with an increased dosage spanning a 3-week period, along with intracavernous PGE1 injection therapy, as a form of treat- ment in 38 patients who had failed to respond to intra- cavernous injection, showed 60% efficiency evaluated by IIEF score.44
8. Other treatments
A number of alternative treatments for erectile dys- function are currently being developed. Topical therapy by application of topical PGE1 to glans penis has received approval from the China Food and Drug Administration and has an efficiency similar to intraurethral PGE1 or MUSE™ but with minor side effects such as a burning sensation at glans penis and penile pain. The topical PDE1 medication that has been preliminarily evaluated is Topiglans by MacroChem. The gel formula consists of 1% alprostadil plus 5% SEPA gel (2-n-nonyl-1,3-dioxolane) that act as a transdermal enhancer. McVary and team has reported an effectiveness of 67-75%.45 Another formula containing 4% Alprostadil gel plus NexAct technology enhancer from NexMed is currently being developed. The dose of 500 mg applied topically was assessed in 10 patients with erectile dysfunction after radical pros- tatectomy by comparing the effects from 10 micrograms dose of alprostadil that were given via intracavernous injection. The measurements of peak systolic, end diastolic activity, and resistive index value were similar to intracav- ernous injection.46
Treatment using gene therapy is predicted to gain popu- larity in the future because of its high effectiveness and elimination of oral therapy or intracavernous injections. The patients would have to visit the hospital to receive an injection of the genes around 3-4 times per year. As the penis is located external to the body, it has slow blood flow when flaccid, so a constriction ring can be applied prior to the injection of the genes, and these factors make the penis a suitable organ for this method of treatment.
Treatment with testosterone has only been used in patients with low testosterone levels. The effectiveness of testosterone therapy for treating erectile dysfunction is low, because low level testosterone is often not the cause of erectile dysfunction but instead is another symptom that can be found with erectile dysfunction. However, testosterone therapy can still help increase bone mass, muscle tone, erythropoietin production, and synthesis of some liver proteins.47
Erectile dysfunction poses as a problem for any sexual relationship and may also affect relationships with family and work. Available treatments for erectile dysfunction are widely accepted with high efficacy, low risks of adverse side effects, and not as complicated compared with previous therapies. Doctors and healthcare workers should learn about the condition in order to be able to provide appropriate consultation to the patients. Selection of treatment uses patient’s goal-directed approach where the patients can select the most suitable form of treatment themselves. Physicians should screen for conditions that may cause erectile dysfunction, for example diabetes mellitus and hypertension, provide recommendations, restrictions, and educate the patients about each form of treatment and make suggestions that match the needs of the patients. When treatment fails, the patients must then be referred to a specialist for further examination and treatment.









