Electronic ISSN 2287-0237
Headache is the primary symptom that brings the patient to see the neurologist. A survey by the World Health Organization (WHO) in 2007 found that the incidence of headache affected up to 47% of the population worldwide.1 These headaches not only cause annoyance but also influence the quality of life.
A survey by David B. Matchar and colleagues2 found that certain types of headache, such as migraine, could cause inability to work in more than 85% of patients. If calculated in terms of direct, economic loss the sum was estimated to be as much as USD 13 billion annually, and WHO had stated that headache was a health problem affecting 1 in 20 working people in the world.3
The International Headache Society (IHS) has divided headache into three groups, namely, 1) Primary headaches, 2) Secondary headaches and 3) Cranial neuralgias, central and primary facial pain, and other headaches.4
Primary headaches are caused by abnormalities of the brain and nervous system itself. No abnormality can be detected by radiological and laboratory tests. Examples of primary headaches include migraine headaches, tension type headache, and trigeminal autonomic cephalalgias (TACs) such as cluster headache, etc.
Secondary headaches are headaches caused by internal or external conditions such as brain tumor, cerebral hemorrhage, cerebral venous thrombosis, head injury, sinusitis, eye disorders, abnormalities of the teeth or temporomandibular joints, infectious diseases, etc. It is necessary for this group to have additional investigations such as Computerized Tomography (CT), Magnetic Resonance Imaging (MRI), and blood tests.
Cranial neuralgias, central and primary facial pain, and other headaches are from other causes. For example, headaches caused by abnormalities of the 5th or 9th cranial nerves or an inflammation of occipital nerves, etc.
Approximately 20% of the patients who visited the Neuroscience Center at Bangkok Hospital presented headaches as a primary symptom. Therefore, the Compre- hensive Headache Clinic has been established and initiated a multidisciplinary team made up of headache specialists, nurses, rehabilitation doctors, physical therapists, clinical psychologists, and medical acupuncturists who can provide comprehensive assessment, treatment and headache education in accordance with international standards.
The aims of the Comprehensive Headache Clinic are to reduce the frequency and severity of the symptoms, offer effective treatments according to international standards, decrease the overuse of pain medications, enhance quality of life, and educate patients and their families so that they are able to take care of themselves and manage their headaches appropriately.5
Pharmacologic treatment
Acute Treatment
1.Acute pain medications are administrated intrave- nously or orally as indicated, according to the standard treatment guidelines from the American Academy of Neurology and European Federation of Neurology Society.6-10
2.Occipital nerve block, Trigger point injection, and/or Peripheral nerve block are performed as indicated.11,12
Prophylactic Treatment
1.Prophylaxis medications are administrated as indicated, according to standard treatment guide- lines from the American Academy of Neurology and European Federation of Neurology Society.6-10
2.Occipital nerve block or Botulinum toxin injection are performed as indicated.12,13
Non-pharmacologic treatments14,15
Headache Impact TestTM (HIT-6TM), the pain score, and the headache frequency per week were used to evaluate the progression of clinical and therapeutic responses in each patient.
Headache Impact TestTM (HIT-6TM) Version 1.115
The test was developed to help patients to communicate their feelings about headache especially in terms of the severity of symptoms and the impact on their daily life. There are 6 questions for patients to answer according to how they feel and the scores will be calculated. The symptoms of headache are divided into 3 levels: Mild score of 50-55 (the headache had a minimum impact on daily life and did not require medical attention), Moderate score of 56-59 (the headache had a moderate impact on daily life and required medical attention), Severe score of ≥ 60 (the headache had severe impact on daily life and required urgent treatment).16 HIT-6TM record form and interpretations are shown in Table 1.
Pain Score
The pain assessment was graded on a numerical rating scale (NRS) with a score of 0-10. There were 4 levels starting from 0 = no pain, 1-3 = mild pain, 4-6 = moderate pain, and 7-10 = severe pain.17
Headache frequency per week
The number of headache attacks per week was asked.
Statistical analysis
Patient characteristics were described as absolute numbers, percentage, mean, and standard deviation (SD).
Inferential statistics was used with Paired sample T-test to determine the headache scores before treatment (Day 0) versus after treatment (Day 28).
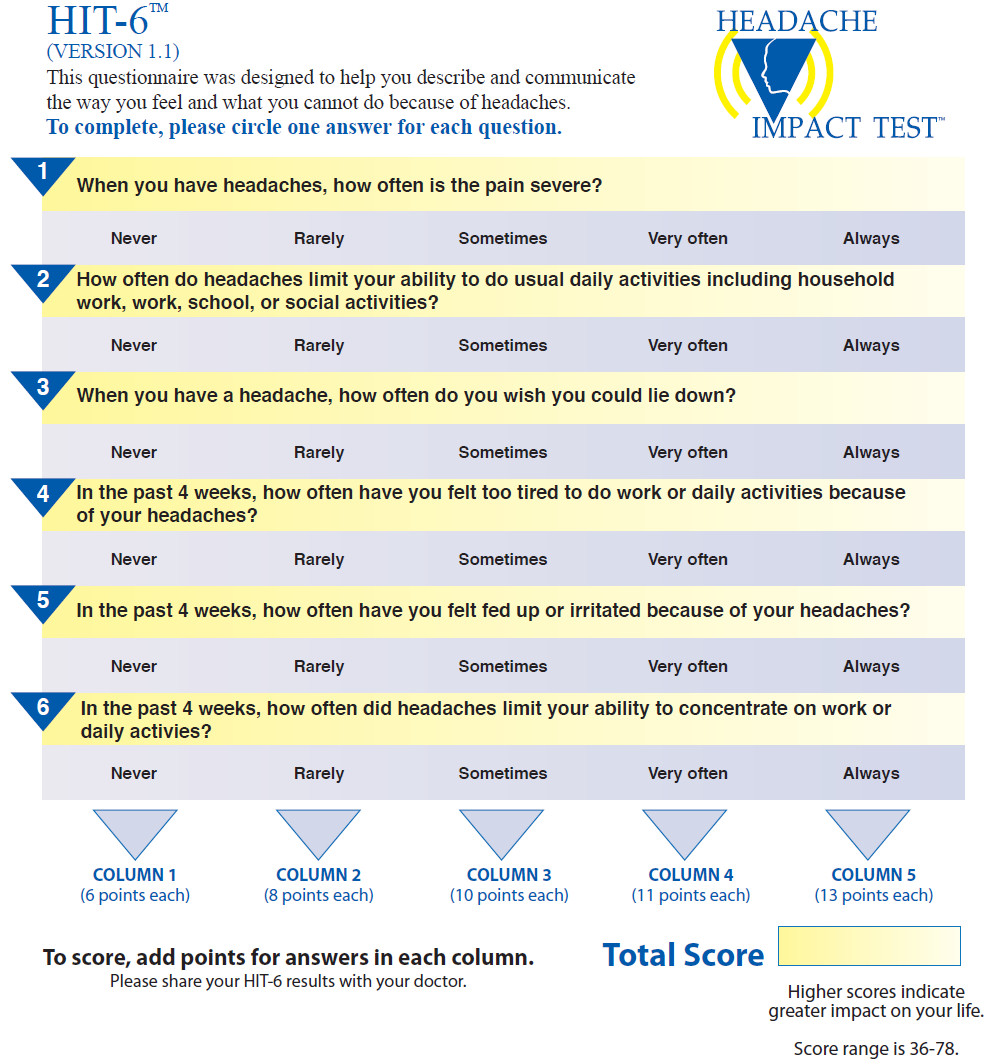
Figure 1: The Headache Impact TestTM(HIT-6TM) form.
Table 1: The Headache Impact TestTM(HIT-6TM) interpretation.
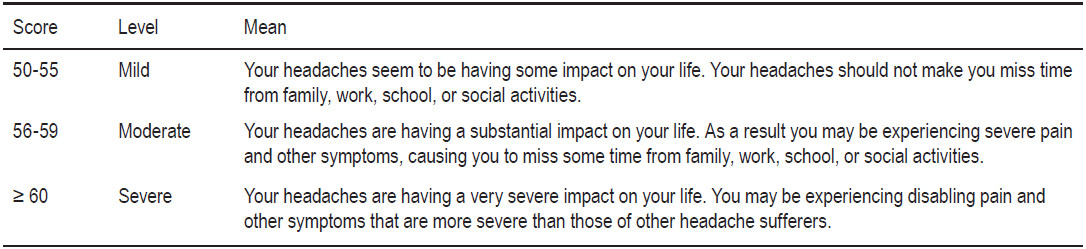
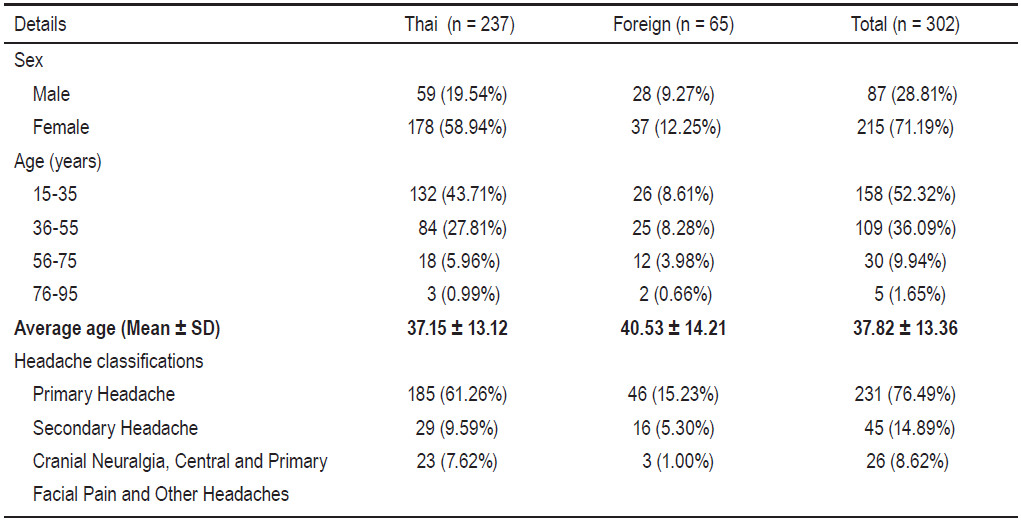
Table 2: Patient characteristics and Headache subtypes
Since the opening of the Comprehensive Headache Clinic at Bangkok Hospital on July 2011 there were 302 patients with headaches that were treated in the clinic during the first 6 months (until January 2012).
Population
Of the 302 patients, 237 (78.5%) were Thai, 65 (21.52%) were overseas visitors, 87 (28.81%) being male and 215 (71.19%) being female. Age range between 15 and 35 years in 52.32% and over 35 years old in 47.68%.
Headaches were classified, according to the Inter- national Headache Society (IHS), into: Primary headache in 229 cases (75.83%): migraine headache 168 cases (73.36%), tension type headache 42 cases (18.34%), other primary headaches 16 cases (6.99%), and cluster headache 3 cases (1.31%).
Secondary headache in 47 cases (15.56%): cervicogenic headache 30 cases (63.83%), medication overuse headache 11 cases (23.40%), and post-traumatic headache 3 cases(6.38%) and other secondary headaches 3 cases (6.38%).
Cranial Neuralgia, central and primary facial pain and other headache accounted for 26 cases (8.61%): occipital neuralgia 8 cases (30.77%), other primary facial pain 7 cases (26.92%), other cranial neuralgia 6 cases (23.08%), and trigeminal neuralgia 5 cases (19.23%). Patient charac-teristics and headache subtypes were shown in Table 2.
From 302 patients, there were 113 cases (37.42%) who completed a four-week followup period. Those that did not come for followup include 111 cases (36.75%) with mild headache that did not require any further treatment; 63 cases (20.86%) did not keep their appointment and when we called to check how they were, they said that their headaches had improved a lot; 15 cases (4.97%) continued their treatment abroad.
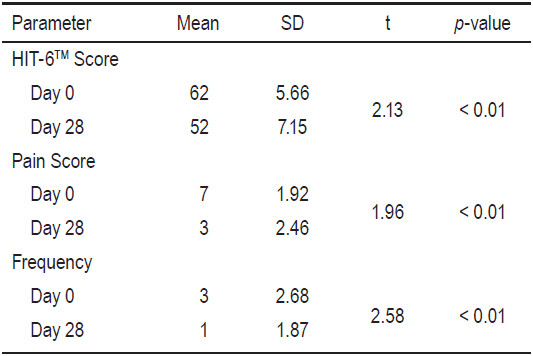
Those with completed a four-week followup were asked to answer three evaluation forms. Comparisons between the first day of treatment (Day 0) and the last day after 4 weeks of treatment, using the Paired T-test, showed a statistically significant decrease in the impact of headache, the severity of headache, and the frequency of headache per week. HIT-6TM Score day 0 = 62±5.66, day 28 = 52±7.15 (p < 0.01, t = 2.13), Pain Score day 0 = 7±1.92, day 28 = 3±2.46 (p < 0.01, t = 1.96), Headache frequency per week day 0 = 3±2.68, day 28 = 1±1.87 (p < 0.01,t = 2.58) (Table 3 and Figure 2).
From our Comprehensive Headache Clinic, on the first day (Day 0) patients had an average headache score (HIT-6TM) of 62 (severe headache impact), average pain score of 7 (severe pain score) and the average headache frequency score was 3 times per week (high frequency). After the 4 weeks treatment of headache, we found that the severity of headache had improved to mild degree and the average headache score (HIT-6TM) decreased to 52 (mild headache impact), the average pain score was reduced to 3 (mild pain score), and the average of headache frequency was reduced to once per week (low frequency). As a result, these patients had a significant increase in their quality of life due to reduced suffering from headaches.
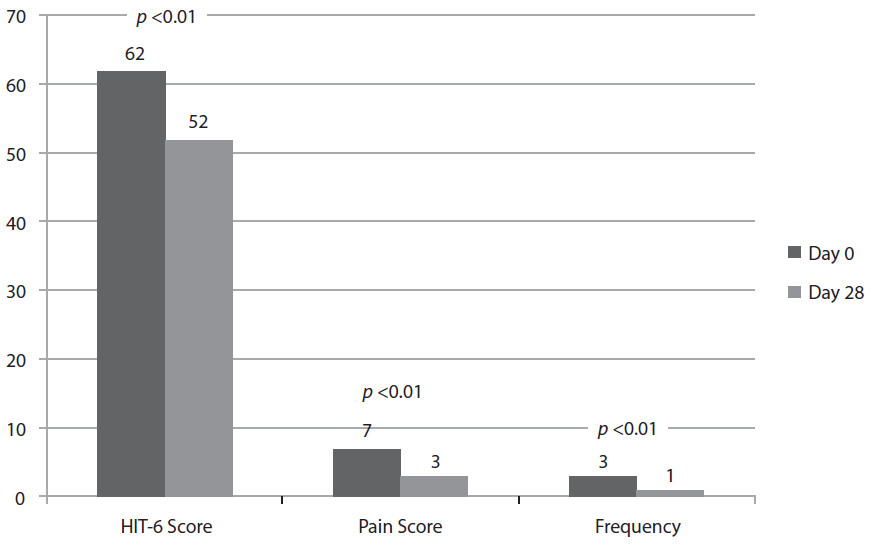
Figure 2: Graph shows the comparison of the headache score on Day 0 vs. Day 28
Table 3: Comparison of headache scores on Day 0 vs. Day 28
Using HIT-6TM score, pain score, and headache frequency per week for treatment evaluation helps patients to communicate more effectively with their physicians. As a result, treatment can be given more effectively and patients can better notice the progression of treatment.
Sauro KM, et al.18 showed in their trial of the Calgary Headache Assessment and Management Program (CHAMP) that the multidisciplinary team were able to significantly reduce the HIT-6TM score from 63.6 to 58.2 (p < 0.001) in three months’ duration.
We propose that by forming a similar Comprehensive Headache Clinic with a multidisciplinary team helps us to improve assessment and treatment of patients with a holistic approach which will accentuate the effectiveness of treatment.
A multidisciplinary team in the Comprehensive Head- ache Clinic can improve the patient’s quality of life by significantly reducing the severity of headache, the frequency, and the impact of headache symptoms. Headache scores will help the patient and physician to reach a common understanding.









