Electronic ISSN 2287-0237
Generally there are three treatment options for replacing missing anterior teeth: removable partial dentures, fixed bridge, and dental implant. To varying degrees, all three options restore chewing function, and provide more normal speaking ability. They also prevent existing teeth from shifting and improve the look of an incomplete smile. The advantages and disadvantages of each of these solutions have been widely discussed in the literature; each treatment option may suit one differently, depending on individual patient’s needs and expectations.
Teeth-supported removable partial denture (removable partial denture)
A well-made removable partial denture is still considered a viable alternative treatment for several patients with multiple missing anterior teeth, especially those with a significant residual alveolar ridge deficiency, medically compromised, and limited financial resources (Figure I).1 Its unnatural feeling and discomfort are the main disadvantages of the removable partial denture.2
Teeth-supported fixed partial denture (fixed bridge)
A fixed bridge is a highly predictable and acceptable treatment option for replacing multiple missing anterior teeth. The predictability of its result is highly dependent on adequate in number and sufficiently healthy of the adjacent (abutment) teeth to support the artificial teeth in the missing area, as well as the patient’s parafunctional activity.2 In order to fabricate a fixed bridge, the abutment teeth are well prepared to reduce their size by removing all the enamel, making room for the prosthetic restoration. Then, a prosthetic (pontic) tooth can be suspended between abutment teeth in this way to provide a functional and esthetic replacement for the missing teeth. However, the limitation with this form of treatment is the permanent loss of tooth structure from the irreversible preparation of abutment teeth (Figure IIA-B). This condemns the patient to the risk of trauma to their nerves. In addition, replacement of fixed bridges often leads to further treatment as the abutment or supporting teeth have been further compromised over time by progressing dental disease such as dental caries or periodontal disease.

Figure I: Replacing multiple missing lower anterior and posterior teeth by removable partial denture.

Figure IIA: Replacing right central and lateral incisors by fixed bridge.
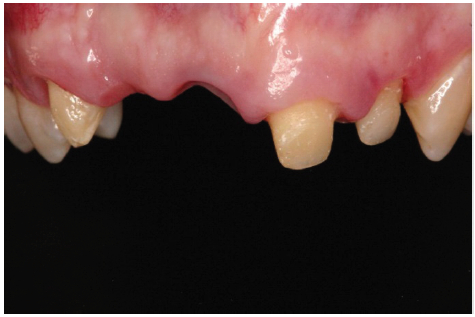
Figure IIB: Several adjacent (abutment) teeth; right canine, left central and lateral incisors, need to be prepared for supporting prosthetic (pontic) missing teeth.
Implant-supported fixed partial denture (dental implant)
Nowadays, dental implants are appealing and are more widely accepted by several patients who have lost multiple teeth, since they offer better alternative options to patients, especially those who are not able to tolerate functionally poor removable dentures.3 Dental implants are also prefer- able for patients who have compromised structural condition and remaining teeth, which would not make good abutments. Still, dental implants are not an alternative treatment for everyone, since patients may require surgery to build up the area needed for the implant, so it is necessary that patients should be in good health in general. There is also evidence showing that heavy tobacco and cigarette smoking may also compromise long term outcomes.3 Patients should be ready to commit to a daily oral care routine and to regular dental visits. The success of dental implants depends on patient knowledge and expectations as well as the care, skill, and judgment of dental clinicians.
Dental implant in highly esthetic areas
The critical goal for esthetic dentistry is to harmonize with the frame of the smile, face and more importantly the individual. Achieving the best results involves comprehensive understanding of the objective and subjective criteria related to hard and soft tissue esthetics since both teeth and gums act together to provide a visual harmony and balance.1
In addition to the dental implants in visible areas, the successful result more specifically depends on the harmony of the crown-implant complex in terms of color and form with the soft tissue surrounding and the neighboring teeth. The predictability of its outcome is very different, and relies on the quality and quantity of the bone and soft tissue. As we know that following teeth extraction, the alveolar bone that supports the teeth tends to remodel over time (resorption), both in width and vertical height of the ridge. This resorption often compromises gingival tissue levels, as the body scallop for the facial to interproximal starts to flatten out, making it very difficult to achieve an excellent gingival scallop if implants are placed. In the so-called esthetic area of the mouth, where loss of ridge and gingival volume can be visibly apparent, this can lead to an esthetic imperfection as well as a higher likelihood to develop food impaction under adjacent teeth (Figure III).4 Proper treatment planning must address hard and soft tissues deficiencies and combine this with precision in implant placement. Advances in bone grafting have made the outcome more predictable.

Figure III: Bone deficiency prior to implant placement on maxillary right central incisor creates compromised soft tissue level and interdental papilla imperfection (black triangle space) between implant and adjacent teeth.
The esthetic outcome of implant restorations are influenced by many variables including:
A. Patient’s expectation and smile line: Patients’ esthetic expectations must be evaluated together with the smile posture. Previous photographs may assist in determining the natural position of the lip when smiling. A high smile line poses considerable challenges because the restoration and gingival tissues are thoroughly displayed. The low smile line is a less critical situation due to the gingival display will be hidden behind the upper lip (Figure IV-V).
B. Implant position: The implants need to be evaluated in three dimensions: apicocoronal, faciolingual, and mesiodistal prior to the surgery since these positions will significantly influence the performing gingival architecture. Placing the implant close to adjacent root creates a great risk of the bone resorption.4 The surgical and radiographic guide along with a computerized tomography scan is essential to evaluate the required precision in implant placement, and to determine the proper diameter size and length of implants.
C. The bony anatomy of the implant site: For successful esthetic restoration, the bony housing must have a three dimensional foundation that permits placement of an implant in a relatively ideal position. The bone graft procedure is necessary if the bony anatomy is inadequate. The most crucial dimension remains the apicocoronal dimension. The patient must understand that the missing hard and soft tissue architecture will need to be rebuilt so that optimum esthetics can be achieved.
D. Implant Restoration: Successful dental restorations on implant in the esthetic area are usually the result of close interdisciplinary cooperation between dental clinicians and technicians. The restorations need to be painstakingly fabricated in the laboratory to mimic the natural translucent appearance. In addition, several issues such as porcelain natural shade layering techniques, precision of margins, accuracy of framework, proper dental anatomy, and optimal occlusion are also a principal focus (Figure VI).5
E. Gingival Biotype: The healthy appearance of the gingiva is a crucial issue. Characteristics of the gingival soft tissue biotype will play a prominent role in the final planning for the implant.4 A thick gingival biotype is more favorable since the thin biotype has a delicate soft tissue curtain, and reduced quantity and quality of keratinized mucosa. Therefore, the thin biotype will require the implant to be placed more palatal and deeper to allow a proper emergence profile and mask any metal show through.

Figure IV: Receded gingival soft tissue level after placing the implant on maxillary right central incisor.
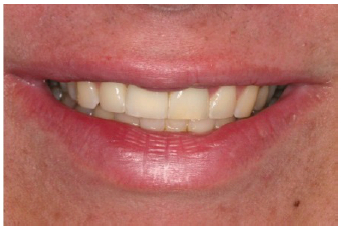
Figure V: The gingival display is hidden behind the upper lip in patient with low smile line creating a satisfactory appearance.
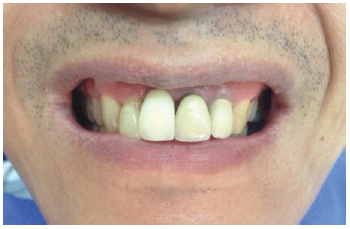
Figure VI: Placing the implant too far apically and the mismatched porcelain natural shade of the implant restoration creates a compromised esthetic outcome on the maxillary right central incisor.
These following cases require close cooperation among the orthodontist, oral surgeon, periodontist, and prostho- dontist. They illustrate how multiple missing teeth can be replaced with dental implants.
A 19-year-old healthy female had several missing teeth congenitally, on the maxillary left and right lateral incisors, and two mandibular central incisors (Figure 1A-B). Orthodontic treatment was complete, and the patient was using a removable retainer with denture teeth attached for the prosthetic replacement of the teeth. The patient was unhappy with the appliance and wanted a permanently fixed solution. The oral examination revealed the edentulous alveolar ridge had a fair amount of bony and gingival architecture. A decision was made for dental implant treatment(Figure 1C-D). Several months follow up revealing interdental papilla levels were increased gradually and improved natural appearance (Figure 1E).

Figure 1A-B: After Orthodontic treatment, patient still has spaces of missing teeth area of maxillary left and right lateral incisors, and two mandibular incisors.

Figure 1C-D: Four implants were placed in the missing area.

Figure 1E: The gingival tissue has a satisfactory natural appearance after several months follow up
A 27-year-old healthy male, lost the maxillary left incisor in an accident 10 years ago. The bony anatomy is inadequate both in width and height due to the resorption after the tooth was extracted (Figure 2A-B).
The bone graft procedure was performed prior to the implant placement (Figure 2C). The final result is esthetically acceptable (Figure 2D).

Figure 2A-B: Inadequate bone width and height for ideal implant position in all three dimensions
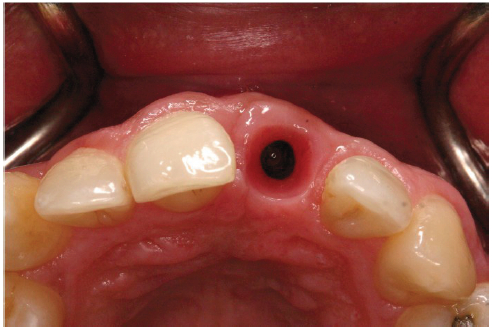
Figure 2C: Optimum implant positioning after the proper bony structure by bone grafting procedure

Figure 2D: Satisfied soft tissue profile and restoration on the implant
A 48-year-old healthy male lost several maxillary teeth from an infection (Figure 3A). The periodontal treatment and maintenance was performed before the patient went through the dental implantation procedure. Following the bone graft, two implants were placed in the precise positioning of the lateral incisor and premolar to support the multiple unit fixed implant prosthesis according to the surgical guide (Figure 3B-D). The patient was very satisfied with the esthetic and functional result (Figure 3E).

Figure 3A: Multiple missing teeth on maxillary left anterior to posterior teeth
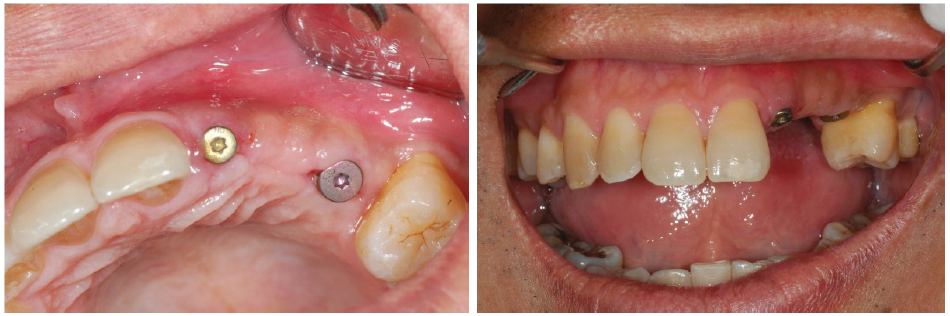
Figure 3B-C: Two implants were precisely placed at the lateral incisor and premolar sites to support a multiple unit fixed implant prosthesis
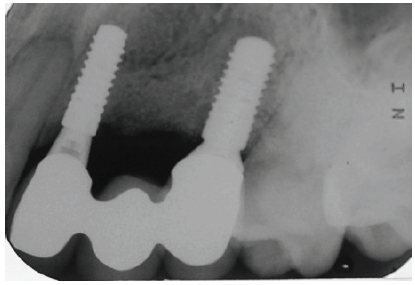
Figure 3D: Radiographic examination revealing precisely parallel placement of implants

Figure 3E: Clinically-acceptable function and esthetic result
The decision of replacing missing anterior teeth must be performed by the dentist and patient after a proper discussion has been had. Common choices would include: fixed bridge, removable partial denture, and dental implants. Each has its advantages and disadvantages. The dental implant itself has several advantages, from its natural appearance, preservation of unrestored adjacent teeth, arresting the resorption of edentulous spaces and optimal support. However, it requires a longer treatment time, a delicate provisional restoration, precise surgical placement and it has a higher cost. Despite these disadvantages, however, a dental implant can be successfully executed when all the factors are addressed: then a dental implant can be considered the treatment of choice for replacing missing teeth.
In the esthetic area, it is critical that the treating dentists and patients are clear about what can be realistically expected and what changes may need to be made in the plan dependent upon the outcome of each phase of treatment. This allows the patient and clinician to proceed with a clear understanding of the potential complications and financial costs. Multidisciplinary treatment and team planning are necessary for the success of implant replacement in esthetically visual areas.
Dr. Pintippa Bunyaratavejon for the periodontal treatment and implant surgery.









