Electronic ISSN 2287-0237
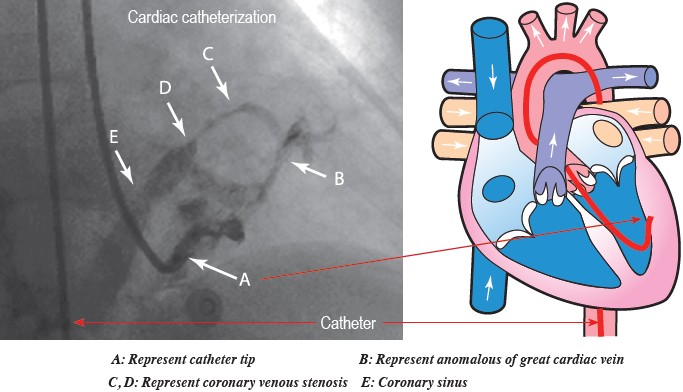
A 77-year-old-woman, a known case of coronary artery disease (CAD), diabetes mellitus (DM) and hypertension developed dyspnea and oppression. She had a history of congestive heart failure, and hyponatemia. This responded well to conservative management. The coronary angiogram showed normal left main coronary artery left anterior descending (LAD) and showed the patent stent at mid LAD. The left circumflex artery (LCX) was normal. The right coronary artery showed proximal focal 30% stenosis. The left ventriculography (LVG) showed Left ventricular hypertrophy (LVH) with good contractility and function ejection fraction (EF) 75%. The tip of the catheter embedded in the left ventricular wall (A) which is proved by injection the opaque media. It filled the cardiac venules, the great cardiac veins (B) and segment of coronary sinus vein stenosis (C, D). The coronary sinus (E) is seen.
Coronary sinus stenosis usually occurs due to iatrogenesis, for instance closure of a secundum atrial septal defect1, late complication of catheter ablation in Wolff-Parkinson-White syndrome or complications of resynchronization therapy.2,3 Reviewing the literature, only one case reported by Rao et al.4 demonstrated absence of the coronary venous sinus without associated structural abnormalities. This is a case of coronary sinus stenosis which is congenital and is associated with anomalous coronary venous fistula.









