Electronic ISSN 2287-0237
The patella plays an important biomechanical role in knee function. Patella injuries constitute up to 1-2% of all fractures, with 70-90% of these having a transverse fracture pattern.1-5 Patella fractures may result in discontinuity of extensor mechanism and potential patellofemoral (PF) joint incongruity.6 As a consequence, effective treatment strategy of patella fractures is essential.
For displaced transverse fracture of the patella, the most commonly used technique is modified tension-band wiring.3, 7-14 The Arbeitsgemeinschaft für Osteosynthesefragen (AO) recommends 15 a modified tension band wiring involving two parallel Kirschner wires and a stainless-steel figure-of-eight wire loop. Nonetheless, various complications have been associated with metal implants in this configuration in 18-50% of patients.12, 16-26 Symptomatic hardware is the most commonly reported complication following fixation of a patellar fracture.12, 16, 17, 25 Lazaro et al.,26 reported 11of 30 (37%) patients with patellar fracture requiring removal of symptomatic implants. Wire breakage and K-wire migration were also reported by several authors.20-24 Other common complications include fixation failure, infection, delayed or non-union, and arthrofibrosis.12, 19, 20
Accordingly, various modifications of tension band fixation have been proposed by using alternative implants in an effort to reduce complications while maintaining fixation strength. 10, 18, 20, 27-36 In place of two parallel K-wires, some authors performed different interfragmentary fixations by using cancellous screws, cannulated screws or bioabsorbable cannulated screws.9, 20, 25, 30, 37-43 Several in vitro9, 39, 40, 43 and clinical studies proved that screw fixation yielded satisfactory outcomes,38, 41 lower painful hardware and implant loosening. 25, 37, 42
For the figure-of-eight loop, several authors have advocated non-metallic implants such as braided polyester. 18, 27, 30-32, 34-36, 43 Clinical studies revealed non-metallic implants provided desirable union rate with lower symptomatic hardware and lower rate of second surgery.18, 31, 32, 34, 36 Another variation includes horizontal orientation of the figure-of-eight loop which was proven to provide better fixation stability, compared to traditional vertically oriented technique.11, 44-46
On the basis of the available evidence, it seems fair to suggest that combining the cannulated screws with horizontal braided polyester loop should provide a strong tension band construct. To our knowledge, there was only one literature focusing on this configuration, which was a biomechanical study in 13 cadavers.43 Bryant et al.,43 compared anterior tension band through cannulated screws using stainless steel wire and FiberWire and found no difference between wire types in fracture displacement and load-to-failure. However, this study did not compare their techniques with the traditional modified tension band technique.
Moreover, heterogeneity of the studies including differences in surgical techniques, knot tying and study designs make it difficult to draw a conclusion on biomechanical aspects of material and fixation techniques. We speculated that the tension band construct using horizontal braided polyester loop and two 4.0 mm cannulated lag screws would provide a strong construct for simple transverse patellar fracture and it might be a useful alternative to the traditional metal implant.
A single finite element (FE) model of the patella was created by using CT images of normal patella. Written informed consent was obtained from the subject. A digital computed tomography (CT) image of uninjured right patella was obtained from an existing CT data of 46-year-old man (weight 70 kg, height 165 cm). A summary of our approach for finite element analysis is demonstrated in Figure 1.
Finite element modelling
1. Transform CT images into three-dimensional (3D) patella geometry
Digital imaging and communications in medicine (DICOM) CT images of patella were imported into Mimics 10.01 (Materialise, Leuven, Belgium) to create a threedimensional (3D) patella geometry. To simplify calculations, all soft tissues, including capsules and ligaments, were excluded.
2. Create solid CAD model for meshing
A 3D patella (.STL) file was imported into PowerSHAPE 2016 (Delcam Plc, Birmingham, UK) to generate a computer aided design (CAD) model to be eligible for meshing. The real curvature of patella surface was transformed into multiple small flat surfaces. The generated model had mean deviation from the real patella at 0.5467 (range -3.098 to 4.914 SD=0.805). Most deviation was at the postero-inferior surface of the patella which would not affect the tension band mechanism.
Fracture and figure-of-eight fixation were also created in this step, and as a gap of
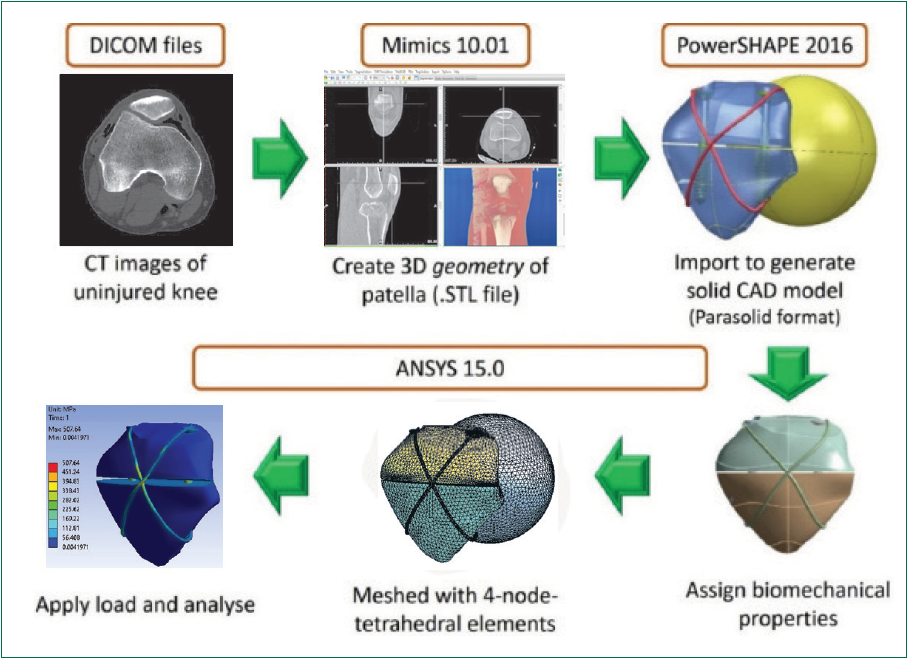
Figure 1: Flowchart of finite element modelling.
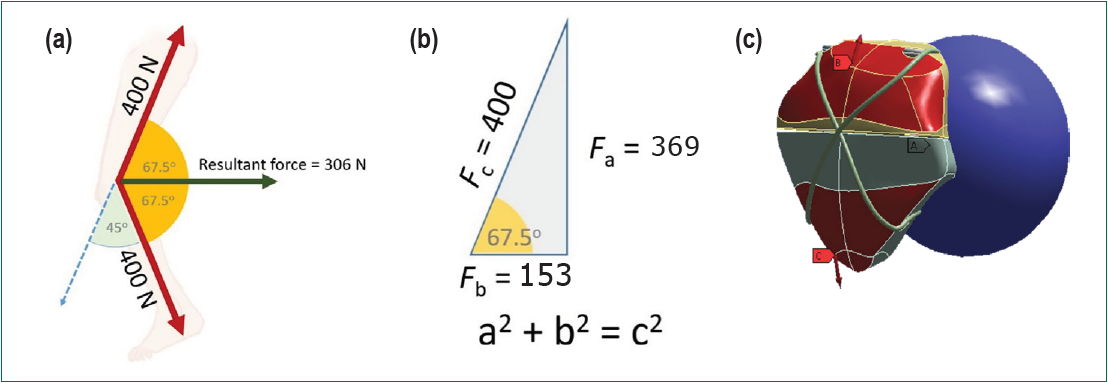
Figure 2:
(a) 1) A 45o knee flexion can be simulated with 67.5o pulling force on each fragment perpendicular to PF joint.
2) 306 N joint reaction force was combined by two of 153 N forces on each fragment with the same vector direction.
(b) Trigonometric calculation of force vectors.
(c) Graphic of patella model in ANSYS 15.0 showing generated pulling force vectors on each fragments. The blue sphere acted as the femoral condyle.
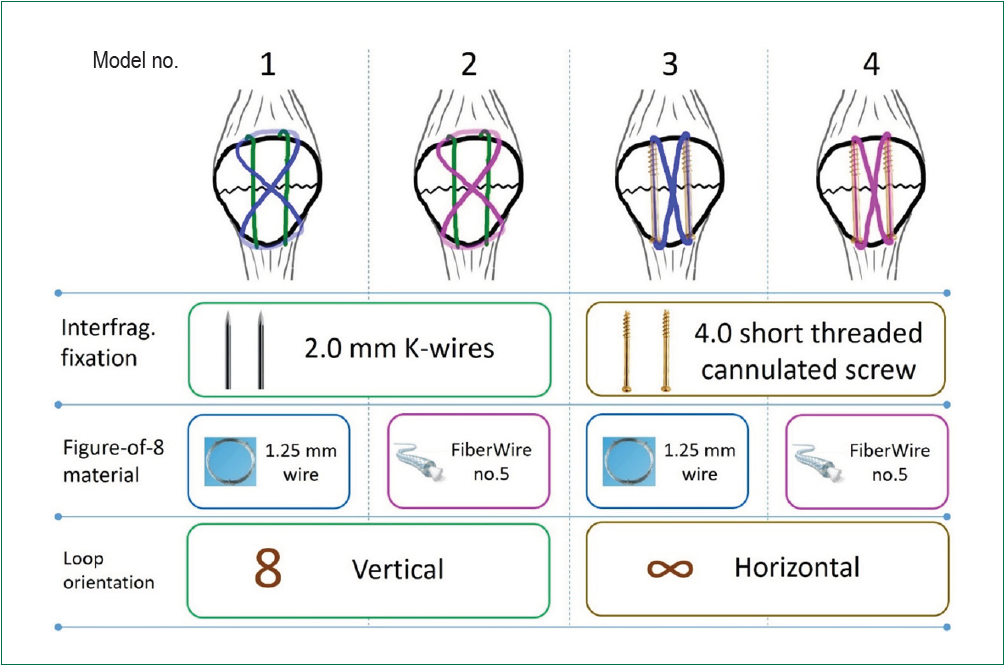
Figure 3: Schematic diagram of tension band configurations which were investigated in our study
3. Meshing
Afterwards, a CAD file was used to mesh a finite element model in ANSYS 15.0 (Ansys Inc, Canonsburg, Pennsylvania, USA). (Figure1). The patella and screw were meshed with 4-node tetrahedral elements. Figure-of-eight wire and braided polyester were in hexahedral elements. All bone and implants were assumed to be homogeneous, isotropic, and linear elastic. Biomechanical properties of bone47, 48 and implants49, 50 were assigned into the models. All metallic implants were 316L stainless steel. 4.0 cannulated cancellous screw’s specification was simulated from Synthe s screw (Synthes GmbH, Oberdorf, Switzerland) having 2.6 mm core diameter and 1.2 mm cannulated diameter. For braided polyester, we used biomechanical properties of FiberWire no.5 (Arthrex, Naples, FL, USA), as it has been proven to offer superior load-tofailure and stiffness comparing to another available suture material.50 Material properties of patella bone,51 316L stainless steel49 and FiberWire no.550, 52 are shown in Table 1.
Table 1. Material properties which were assigned to each model

4. Boundary condition, load application and analysis
The placement of figure-of-eight loop was close to the bone, as the tension band became more stable while turning over adjacent bone surface.45 The sphere acting as femoral condyle contacted the posterior surface of the patella. We attempted to create an environment as close to the actual physiological condition as possible. The PF joint reaction was maximum at 45o 6 and 400 N is required to get full knee extension,43 so we simulated a 45o knee flexion. The loading forces on each fragment were equivalent at 400N and 67.5o relative to the axial plane in order to get a resultant force perpendicular to the joint. To create the pulling force of 400 N on each fragment, we differentiated the vectors. The longitudinal pull (a) was 369.6 N, the transverse pull (b) was 153.1 N. (Figure 2a-c).
5. Model validation
The promoted finite element model was validated by comparing the simulation result prior to the biomechanical experiment. Carpenter et al.,9 found that the traditional modified tension band with metal implants failed at 395 N (SD = 147). Our similar construct (model 1) demonstrated tension band failure at 400 N. which was comparable to Carpenter et al., 9 study.
The calculated results are demonstrated in Figures 4-5. The least von Mises stress (Figure 4) was found in model 4 (cannulated screws with FiberWire; 471.2 MPa) whereas model 1 was subjected to the most stress (all metal implants; 1422.9 MPa).
By using the 4.0 mm. cannulated cancellous screw for interfragmentary fixation (Model 3&4), the stress on the implant reduced by three times comparing to the use of K-wires (Model 1&2). The total material deformation in the screw groups were also less than those of K-wire groups (Figure 5).
Considering the implant for figure-of-8 loop, both the stainless steel wire (Model 1&3) and FiberWire (Model 2&4) provide similar stress on the implants and at the fracture site.
Regardless of the implant or fixation techniques, all models demonstrated that the von-Mises stress distribution was mainly on the figure-of-8 loop with peak stress found at the crossing junction of the loop.
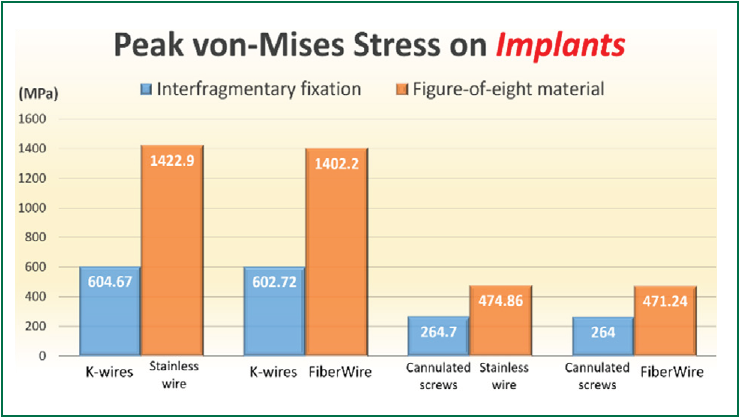
Figure 4: Peak von-Mises stress at interfragmentary implant and figure-of-8 loop on each model. At figure-of-eight loop, stainless-steel and FiberWire sustained comparable stress on the implant.
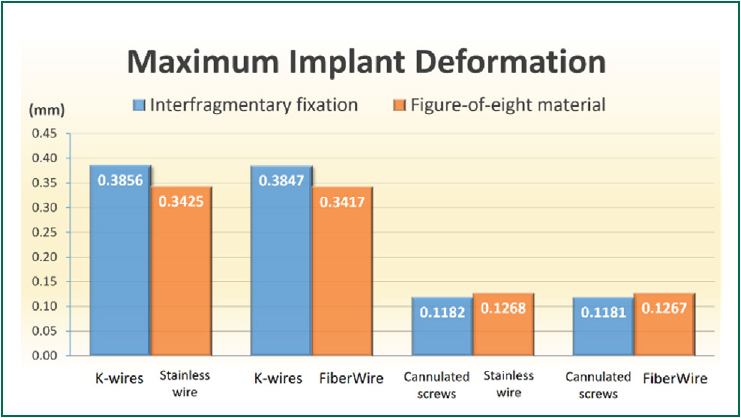
Figure 5: Maximum implant deformation upon loading. By using cannulated screws as interfragmentary fixation, all implant construct deformed 3x less than using stainless-steel wires.
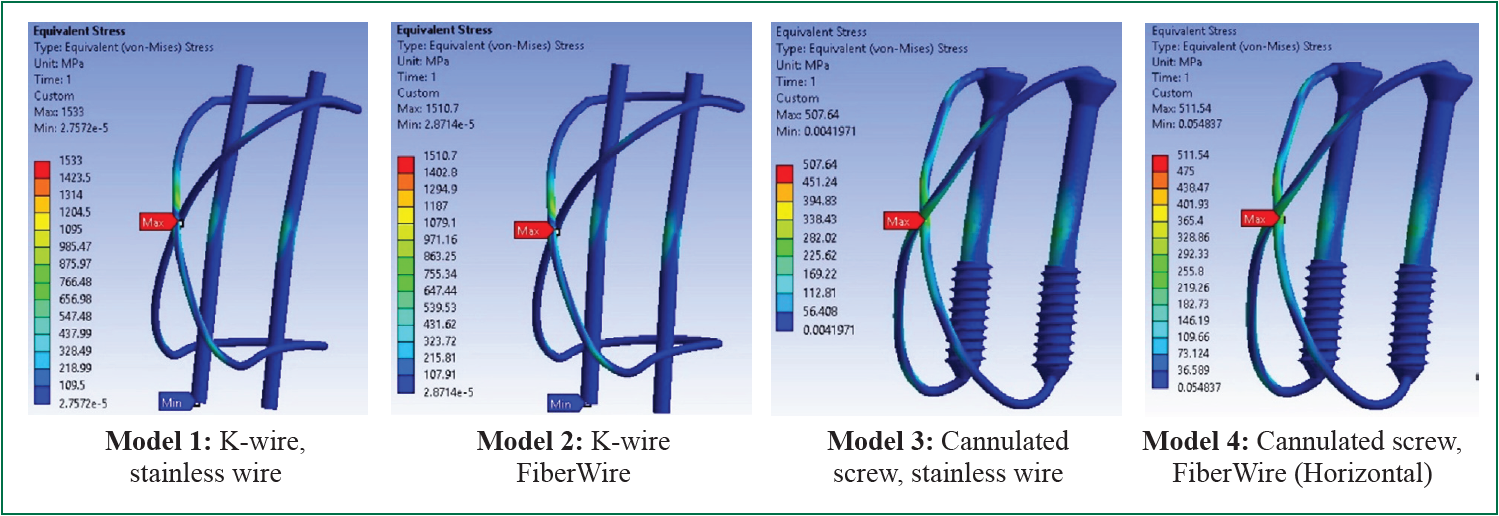
Figure 6: Distribution of von Mises stresses on the implants. All models have peak stress at the crossing junction of figure-of-8 loop.
In this biomechanical study, our primary objective was to compare the biomechanical strength of modification of tension band construct. According to our literature review, this is the first finite element analysis (FEA) study on tension band fixation. FEA has now become widely accepted as a noninvasive and excellent tool for studying the biomechanics and the influence of mechanical forces on biological systems. It is a mathematical tool, which relies on the simplification of complex situations into a number of discrete, smaller problems.53 For our study, the principal advantage of FEA is elimination of potential confounding factors which might be encountered by other types of biomechanical studies, such as the cadaver’s bone and soft tissue condition, uniformity of created fracture, and quality of knot tying. It enabled us to stipulate the theoretically ideal condition for implant fixation. However, it has to be accepted that the strength of braided polyester tension band also depends on knot tying technique issues.11, 29, 44, 46, 54, 55 Clinical application of braided polyester needs to consider the knot tying issue.
To simulate the knee environment, prior cadaveric studies applied the traction on the cadaver’s quadriceps muscle 9, 10, 40, 43 and flexion of knee cadavers created actual patella gliding mechanism. Patellofemoral joint is subjected to dynamic stress. The fulcrum for bending moment migrates proximally with greater degrees of knee flexion.56 The joint reaction force was also affected by lateral force from Q-angle effect.57 As simplifications are necessary during finite element modelling,53 simulation of this complex movement might make the FE model unreliable. In accordance with biomechanical studies under synthetic model setup,11, 44, 58 we simulated a three point bending model with a sphere acting as a femoral condyle.
Interfragmentary fixation: K-wires, cancellous screws or cannulated cancellous screws
Prior clinical studies reported that to limit cerclage wire migration, the Kirschner pins must protrude into the patellar and quadriceps tendon and are often bent.16, 59 K-wire protrusion into the patellar and quadriceps tendon may cause local tissue irritation, inhibits motion and subsequently requires implant removal.16, 59, 60 As these tissues atrophy, cyclic loading causes wire loosening with subsequent loss of fixation strength. Modifications of interfragmentary fixation include cancellous and cannulated cancellous screws. Biomechanical studies demonstrated that screws provided more stability compared to parallel K-wires.8, 9 According to Burvant et.al.,40 screws provide interfragmentary compression throughout the range of motion and resist tensile loading at terminal extension. Moreover, the screws further serve as tension band during the 40-60o of flexion which produces maximum eccentric loading to the patella. 40 In a cadaveric study, Carpenter et al.,9 proved that combining interfragmentary screw fixation with tension band wiring through the screw’s cannulation failed at the highest static load. Several clinical studies 30, 37, 38 provided confirmatory evidence of successful outcomes with cannulated screw and tension band construct through the screw’s cannulation. Hoshino et al.,25 also observed that patients treated with K-wires were twice as likely to undergo implant removal compared with those treated with screws.
Our results demonstrated that the implant stress and deformation were less on the model with screw fixation. This could be a positive effect from the screw resistance to bending movement, which is better than K-wires.61
Implants for figure-of-eight loop: Stainless-steel wire or braided polyester
As a substitute for stainless steel wire in making a figureof- eight loop, previous studies advocate the use of non-metallic implants.10, 18, 29-33 Braided polyester has been one of alternate choices as it offers mechanical advantage to other nonresorbable and resorbable sutures in vitro, combining properties of high stiffness and high ultimate tensile strength.62 There was a perception that such suture material was weaker than steel and might provide a weak tension band construct. Biomechanical studies proved that braided polyester provides sufficient or superior stability in a tension band fixation.10, 28, 29, 55, 58 The resultant advantage of using suture material, as shown in clinical studies to date, is less frequent hardware complications. 18, 27, 30-32, 34-36 Gosal et al.,18 compared stainless steel wire with braided polyester material. The relative risk of re-operation in the metal group is six times that of the non-absorbable suture group (38% to 6%) and a higher infection rate in the former has significant implications on patient morbidity. A systematic review, by Camarda et al.,63 showed that non-metallic implants are able to deliver good clinical outcomes reducing the rate of surgical complications and re-operation. Bryant et al.,43 has investigated a combination of stainless-steel or FiberWire with cannulated screw. His resulted showed that there was no difference between wire types in fracture displacement and the load to failure. He concluded that FiberWire provides similar protection to steel wire against repair displacement after fixation of patellar fractures.
Our results showed that stainless-steel wire and braided polyester for tension band offers comparable implant stress, strain and deformation in both K-wire and screw groups. This result corresponds to a recent study by Bryant et al.,43
Horizontal figure-of-eight loop: a proven better configuration
In making the tension band construct, classic figure-ofeight configuration is a vertical oriented wire curving anterior to the patella and passing under quadriceps and patella tendons. 15 Comparing with classic vertically oriented technique, horizontal figure-of-eight loop provides greater interfragmentary compression.11, 44, 45 Recent clinical studies found that a horizontal figure-of-eight wire loop resulted in a lower postoperative complication rate.46 Interestingly, all research involving cannulated screw constructed a tension band with horizontal figure-of-eight loop through the screw’s cannulation. 9, 20, 30, 37, 38 This raises a conflicting issue of the mechanical stress which may concentrate at the sharp corners as the wires exit on both ends of the screws. Carpenter et al.,9 pointed out that this effect could be minimized by leaving the screws flush with or short of the end of the patella. On our FE model with cannulated screw, we have placed the screw’s head and tip flushed into the bone. Stress analysis revealed minimal stress at the sharp turns of the figure-of-eight loop in both stainless and FiberWire model. Regarding the comparison to the vertical loop, it was difficult to conclude the superiority of horizontal loop (model 3&4) over vertical loops (model 1&2) since there were also differences in implant types. We did not simulate a cannulated screw with vertical figure-of-eight loop since it needs simulation of quadriceps and patella tendon and we designed not to include soft tissue conditions in our study.
Overall treatment cost
Comparing to classic modified tension band wiring, cannulated screw and braided polyester combination has an undoubtedly higher implant cost. Nevertheless, the low profile construct of FiberWire has been proven to offer lower reoperation and infection rates.18 Thus, overall treatment cost could be lower by using the authors’ proposed construct.
There are some limitations to our study. The first is the nature of the finite element analysis method, which lacks a physiological environment and various muscle forces.
The actual bone-implant frictional force could dynamically change by periosteum or soft tissue interposition upon healing process. Secondly, we simulated a static load only at 45oof knee flexion and did not use another angles of knee flexion, which could occur in a real life situation. We did not perform a cyclic loading test, which implants become subject to cyclic bending forces as the patient begins to mobilize.61 Further research in this area including cadaveric studies may validate and extend our results into clinical use.
At 45o knee flexion, tension band combination of two cannulated lag screws and horizontal FiberWire figure-of-eight loop has favorable implant stress, three times less than the traditional modified tension band construct and least implant deformation. Our findings demonstrate superior stability and resistance to fixation failure of the construct. The authors advocate that this low-profile tension band fixation could be a good alternative for transverse patella fracture given that it provides lower hardware complication.
No conflict of interest.









