Electronic ISSN 2287-0237
Clinical manifestations of atherothrombotic disease, cardiac arrhythmia and myocardial infarction account for the most common causes of sudden, unexpected death in all age groups.1 A multicenter study of cardiac death in Thailand showed that of the NSTEMI 2653 cases, cardiac death were 202 cases (7.6%).2
Atherothrombosis is a complex, inflammatory process that begins at the site of endothelial cell injury and culminates in atherosclerotic lesion disruption with superimposed thrombus formation. Consequently it leads to acute coronary syndrome. State of the art treatments of acute coronary syndrome include balloon angioplasty with coronary artery stenting, which show evidence for reducing mortality and improving quality of remaining life in coronary artery disease patients.
However, despite advances, we still face limitations, especially in dealing with particularly large thrombus in a long segment of epicardial coronary artery thrombosis. We presented a case report, which detailed our management of this challenging situation at Bangkok Heart Hospital.
A 69-year-old man, a Marathon runner came to Bangkok Heart Hospital early morning at 4 a.m. due to chest pain at mid-sternal chest. The chest pain radiated from mid-sternal to upper anterior chest wall with the patient reporting a feeling of more heaviness and tiredness a few hours later. At the emergency room, initial electrocardiography (ECG) showed left ventricular hypertrophy (LVH) with elevating ST-T in leads II, III, AVF. Troponin-T and CK-MB were also positive for myocardial damage.
He was sent to cardiac catheterization laboratory immediately after Acute Coronary Syndrome (ACS) pathway was activated. The coronary angiogram showed total occlusion at mid right coronary artery (RCA) (Figure A). Ad hoc Percutaneous Coronary Intervention (PCI) proceeded after the patient’s relatives had been notified and given their permission.
After wiring through total occlusion RCA distally, the subsequent coronary angiogram showed a large thrombus from mid to distal RCA. The interventionist did not attempt further manipulation but preferred to administer low molecular weight heparin (Enoxaparin®) to the patient and kept the patient monitored in the coronary care unit (CCU).3,4
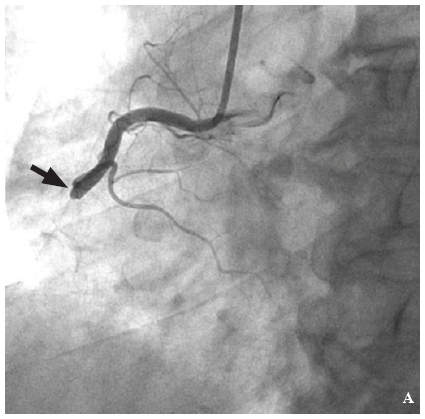
Figure A: Total occlusion at mid right coronary artery (arrow).
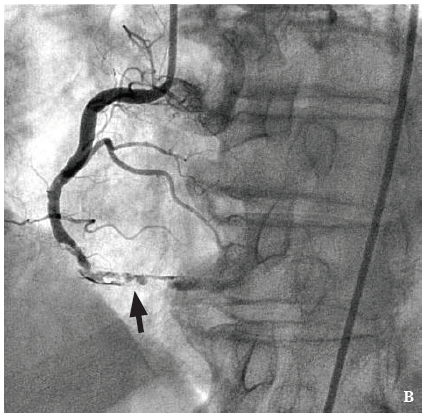
Figure B: Partial thrombolysis at mid right coronary artery and large thrombus distally after 10 days of Enoxaparin.

FigureC: Completely thrombolysis throughout right coronary artery after continue at Enoxaparin and other 10 days.
Fortunately, The patient was stable both mechanically and electrically. It was then decided to administer enoxaparin 60 mg twice daily for 10 days. The scheduled repeated coronary angiogram after 10 days of low molecular weight heparin showed partial thrombolysis at mid RCA and the large thrombus in distal RCA remained (Figure B).
With the patient in a stable condition, no longer complaining of chest pain or tiredness, we planned to continue administering the low molecular weight heparin was for a further 10 days. On the 20th day after first administration of enoxaparin, yet another coronary angiogram was done, which showed completely thrombolysis throughout RCA (Figure C).
Currently, thrombus aspiration prior to balloon angioplasty and stenting are the standard techniques. Unfortunately, it is difficult to eliminate huge thrombus in the large artery. This kind of lesion represents a substantial risk with both short and long term complications, which can include peri-procedural myocardial infarction, distal embolization and long term re-occlusion. Many cardiac centers reported performing minimal manipulation to restore blood flow in cases of large arterial thrombosis.4-6 Low molecular weight heparin, one of the most preferred interventional pharmacotherapies, is frequently used to prevent and treat arterial and venous thrombosis. It works by inactivating thrombin in thrombotic process as well as stopping the formation of fibrin, a significant component of blood clots. In this case report, low molecular weight heparin was the medication of choice. Usually for general thrombolysis, enoxaparin for 7-10 days is adequate to give a good result, restoring blood flow. But for a large thrombus such as in this case study, a longer duration of enoxaparin administration to establish normal blood flow is recommended.7
Extensive coronary artery thrombosis is a difficult problem to handle. Where standard interventions were not obviously adequate to restore coronary perfusion, we report the successful use of a common drug, heparin to establish normal flow in a large long segment coronary artery thrombosis.
In summary, appropriate dosages of low molecular weight heparin and longer duration of administration (up to 3 weeks) is one of the alternatives to consider.









