Electronic ISSN 2287-0237
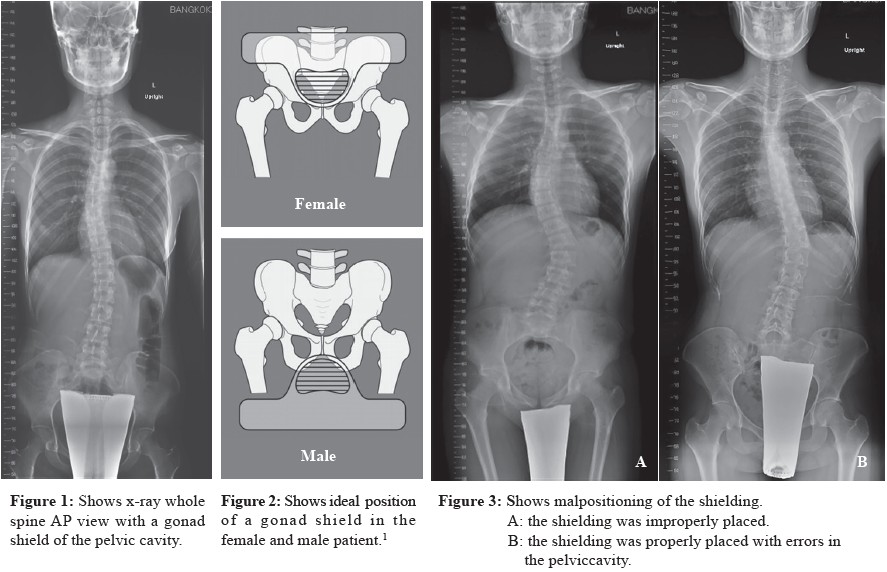
Nowadays, whole spine radiographs are commonly evaluatedtools for scoliosis patients in diagnostic and follow upradiographs. A standing position is mandatory for imageacquisition of the whole spine; C1 down to sacrum. The images arelater fused into only one image (Figure 1).
Radiation shielding at the pubic area is the most concerning afterseveral radiographs are taken, especially in teenager or puberty patients(Figure 2).1
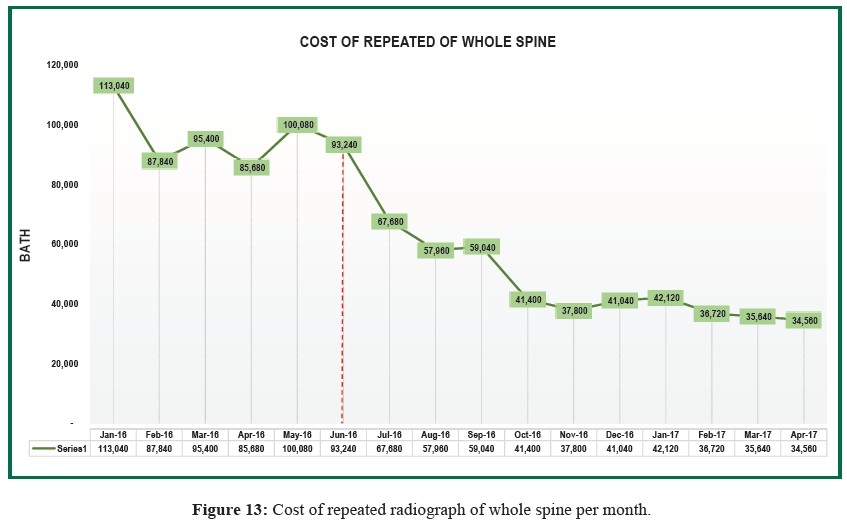
According to the database of the Department of Radiology, BangkokHospital Headquarters in 2015, there were some incidences of repeatedradiographs as follows: whole spine radiographs 39%; knee radiographs33%; chest radiographs 20%; abdomen radiographs 1%; and others 7%.The repeated whole spine radiographs is a double radiation dose, raisingthe cost to 103,016 baht/month on average, and rising the procedure timeby 3 minutes; approximately 75% of the routine procedure time (routineprocedure time is 4 minutes).
The causes to the problems found in repeated radiographsare as follows: 11% patient motion, 29% patient positioningerror, and 60% malpositioning of the shielding (Figure 3).Patient safety is the key of universal patient care. As a result,a new innovation of radiation shielding of the pubic area wasinvented in our department for whole spine radiographs.
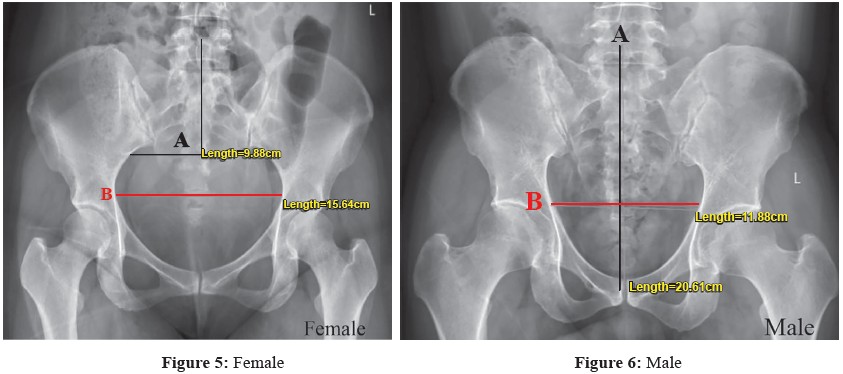
The most common material of radiation shielding is leadplate. The inverted triangular shape is suitable for radiationshielding of the pubic region in both male and female patients(Figure 4).2 The size of the new lead plate was calculated fromthe average measurement of the distance between the medialrim of the bilateral iliac wings; the widest point, in both sexesfrom the pelvis AP radiograph. Also the length of the handlingshielding was measured from the average distance of the iliaccrest to the superior rim of the pubic symphysis for males, andto the widest point of the pelvic cavity for females, from thepelvis AP radiograph (Figure 4).
The radiation shielding, the inverted triangular lead plate,was attached to a rubber belt at the upper rim, to be placed atthe iliac crest of patients. The x-ray beam can pass through therubber belt, and resulted in no artifact on the radiographs.
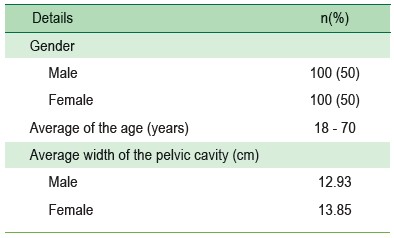
We reviewed 200 pelvic AP upright radiographs, half maleand half female, with an average age between 18 and 70 years(Table 1), to measure the width and height as mentioned aboveand to calculate an average measurement:
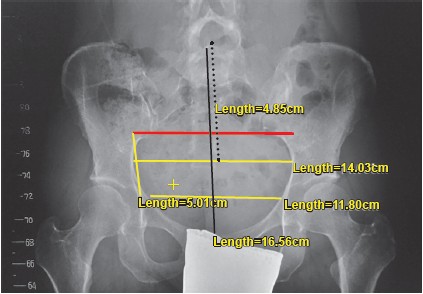 Figure 4: Shows the measurements taken for the new innovative shielding
Figure 4: Shows the measurements taken for the new innovative shielding
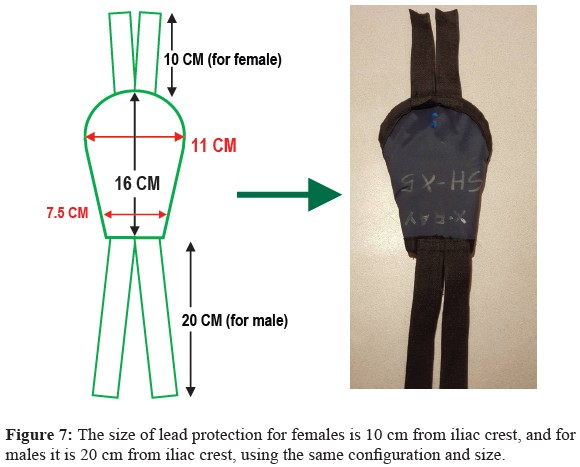
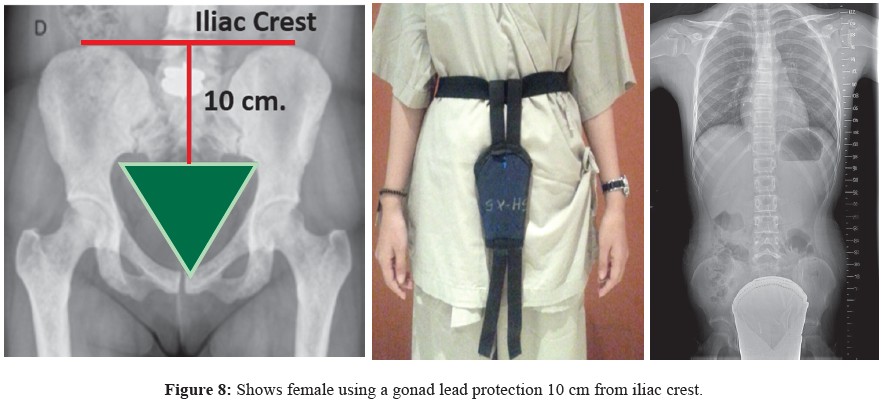
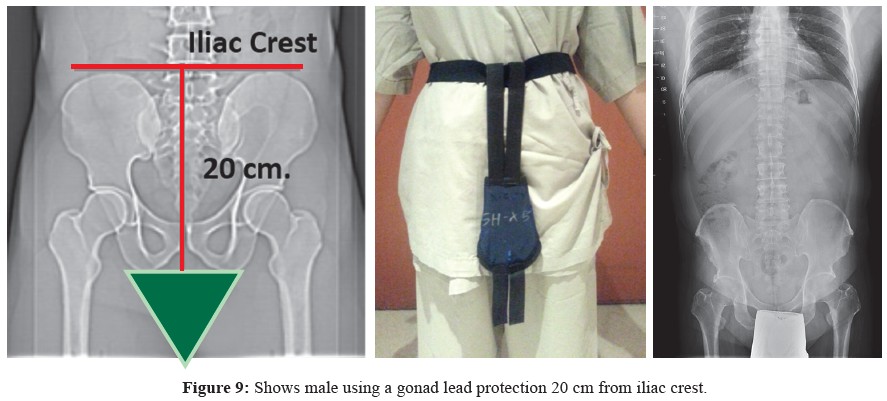
The thickness of the inverted triangular lead plate shieldingwas about 0.5 mmPb demonstrated a radiation transmissiononly 0.4-2.2%3 which was a shielding, standard value, then,covered by cotton, and oil shielding for water resistance. Twosizes of rubber belt for the shielding were made; 10 cm and20 cm for female and male respectively. The bilateral rims ofthe shielding were then folded inside by 1.5 cm. each, avoidingthe hip joint overlap (Figure 7). The iliac crest was the guideused to adjust the position of the lead plate, holding on themidline (Figure 8).
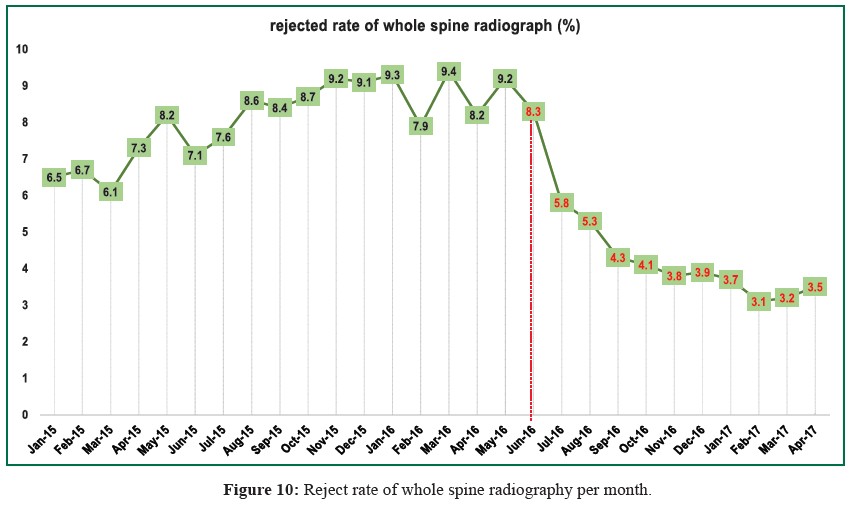
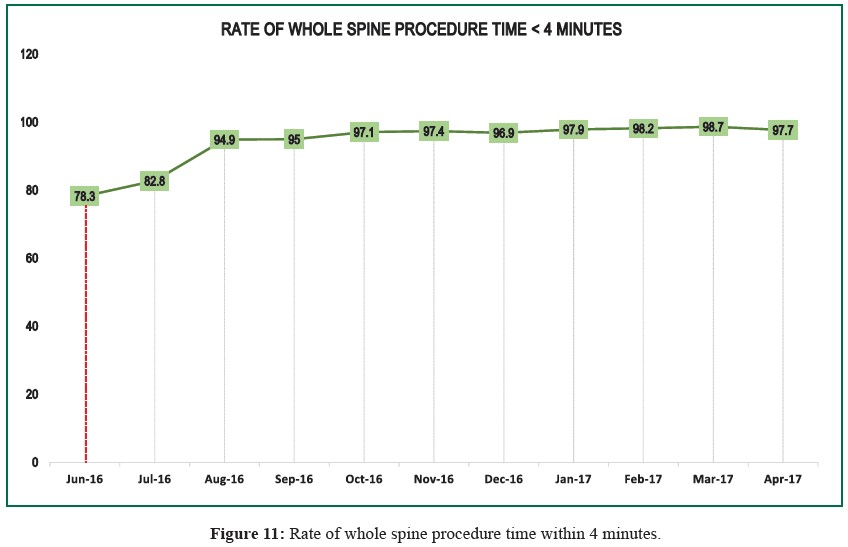
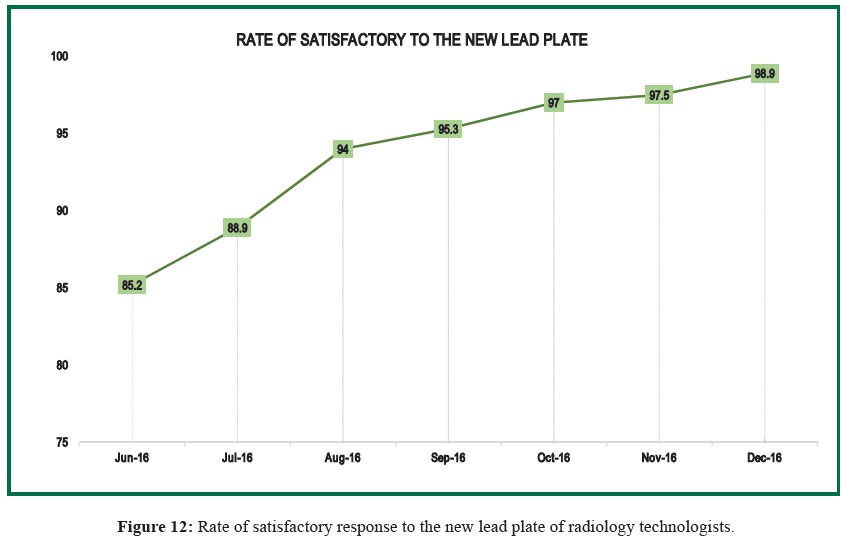
The new lead plate was used in routine whole spineradiographs from June 2016 to April 2017, then repeatedradiograph (rejected rate) was recorded. Rate of routineprocedure time within 4 minutes was recorded from June 2016to April 2017. Rate of satisfactory response to the new lead plateby radiology technicians was recorded from June 2016 to December 2016. The cost of repeated radiograph of wholespine (expense) was also recorded from January 2016 to April2017.
Table 1: Patient characteristics at baseline (n=49)
In children and young adults, gonads are extremely sensitiveto radiation exposure. Rowley MJ, et al. 4 reported the effectof graded doses of ionizing radiation on human testes. Dosesare 10-15 rad (0.01 to 0,015 Gy) can induce depression ofspermatogenesis and the dose of more than 500-600 rad islikely to induce permanent sterility. In young girls, doses of500 rem (5Sv) destroy germinal epithelium.5 The averagetotal permissible gonadal dose per year was 0.013 rads formales and 0.035 rads for females.6 In all circumstances,radiation protection with lead shielding protection is importantand needs to be in the proper position in either male or femalepatients. The positioning of the shielding should be confirmedas satisfactory for the patient’s physician including theradiologist, chiropractor, and orthopedic physician. An adequateshielding should include the entire gonads in male and female.As these are different, female gonads are in pelvic cavity, hencethe protection shield should cover the whole pelvic cavity inwomen, but it should not interfere with interesting structuressuch as the acetabulum and/or hip joints.1,2
We present a lead shielding for gonads in both genders incase of whole spine study in the positioning and fixation ofthe protection in place. We present an analysis of the rate ofrejection, time procedure and expense. We found that the rateof rejection is less than 5%. Routine time procedure is 4 minutesachieving 97% rate, and the rate of satisfactory response interms of fixation and being user-friendly is 95-98%. Theexpense cost of repeat examination decreased by 65% in tenconsecutive months. From this study and analysis, werecommend the use of lead gonads shielding protection as perour configuration and size including male and female sizes aswell as following our positioning protocol in the standingposition. This innovative significantly reduces the rate ofrejection, and the time this procedure takes. It is user-friendlyand reduces expense.
The new inverted triangular lead plate for radiation shieldingis an effective tool as it decreased the rejected rate, decreasedprocedure time, increased satisfactory response of radiologytechnologists and decreased expense. We strongly recommendthis plate for routine whole spine radiographs over theconventional or commercial lead plate.









